

Postoperative Ultrasound, Unassisted Maturation, and Subsequent Primary Patency of Arteriovenous Fistulas
- PMID: 30139806
- PMCID: PMC6140570
- DOI: 10.2215/CJN.02230218
Postoperative Ultrasound, Unassisted Maturation, and Subsequent Primary Patency of Arteriovenous Fistulas
Abstract
Background and objectives: Postoperative ultrasound is commonly used to assess arteriovenous fistula (AVF) maturation for hemodialysis, but its utility for predicting unassisted AVF maturation or primary AVF patency for hemodialysis has not been well defined. This study assessed the predictive value of postoperative AVF ultrasound measurements for these clinical AVF outcomes.
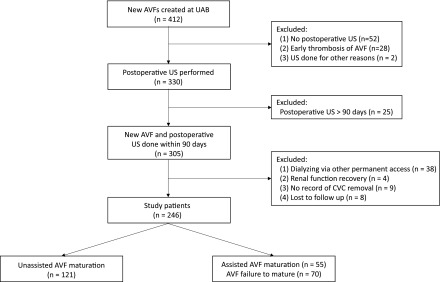
Design, setting, participants, & measurements: We queried a prospective vascular access database to identify 246 patients on catheter-dependent hemodialysis who underwent AVF creation between 2010 and 2016 and obtained a postoperative ultrasound within 90 days. Multivariable logistic regression was used to evaluate the association of clinical characteristics and postoperative ultrasound measurements with unassisted AVF maturation. A receiver operating characteristic curve estimated the predictive value of these factors for unassisted AVF maturation. Finally, multivariable survival analysis was used to identify factors associated with primary AVF patency in patients with unassisted AVF maturation.
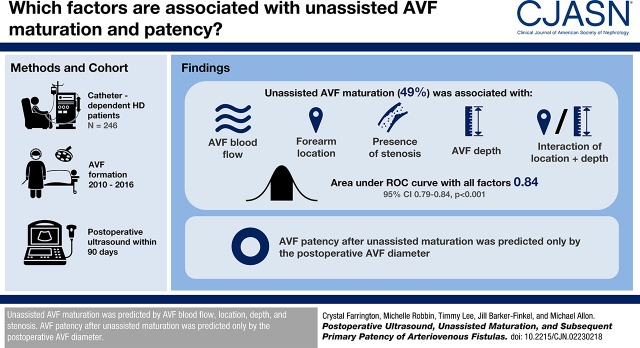
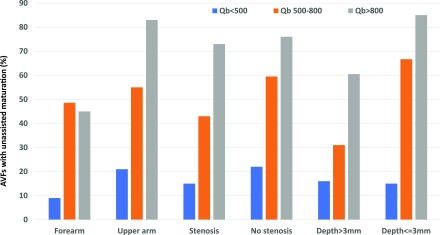
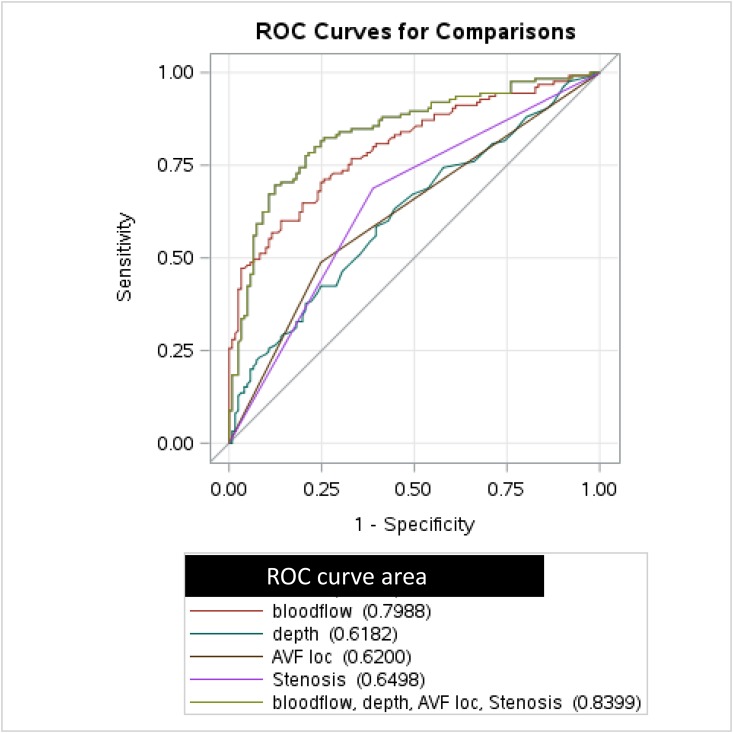
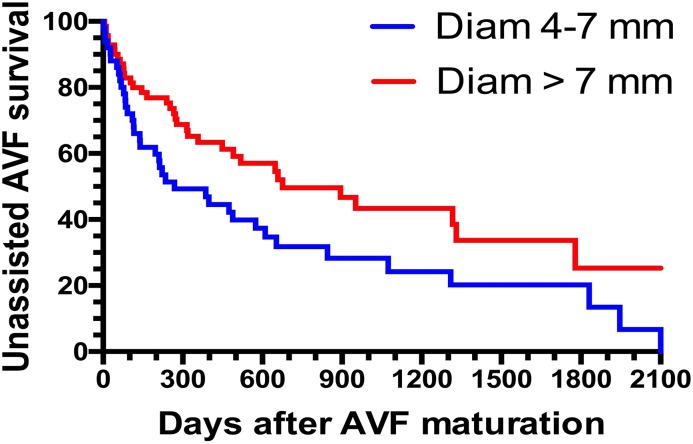
Results: Unassisted AVF maturation occurred in 121 out of 246 patients (49%), assisted maturation in 55 patients (22%), and failure to mature in 70 patients (28%). Using multivariable logistic regression, unassisted AVF maturation was associated with AVF blood flow (odds ratio [OR], 1.30; 95% confidence interval [95% CI], 1.18 to 1.45 per 100 ml/min increase; P<0.001), forearm location (OR, 0.37; 95% CI, 0.08 to 1.78; P=0.21), presence of stenosis (OR, 0.45; 95% CI, 0.23 to 0.88; P=0.02); AVF depth (OR, 0.88; 95% CI, 0.77 to 1.00 per 1 mm increase; P=0.05), and AVF location interaction with depth (OR, 0.50; 95% CI, 0.28 to 0.84; P=0.02). The area under the receiver operating characteristic curve, using all these factors, was 0.84 (95% CI, 0.79 to 0.89; P<0.001). Primary AVF patency in patients with unassisted maturation was associated only with AVF diameter (hazard ratio, 0.84; 95% CI, 0.76 to 0.94 per 1 mm increase; P=0.002).
Conclusions: Unassisted AVF maturation is predicted by AVF blood flow, location, depth, and stenosis. AVF patency after unassisted maturation is predicted only by the postoperative AVF diameter.
Keywords: Constriction, Pathologic; Forearm; Humans, ROC Curve; Logistic Models; Prospective Studies; Survival Analysis; arteriovenous fistula; hemodialysis access; renal dialysis; vascular access.
Copyright © 2018 by the American Society of Nephrology.
Figures
Comment in
-
Determinants of Arteriovenous Fistula Maturation.Clin J Am Soc Nephrol. 2018 Sep 7;13(9):1307-1308. doi: 10.2215/CJN.08860718. Epub 2018 Aug 23. Clin J Am Soc Nephrol. 2018. PMID: 30139805 Free PMC article. No abstract available.
References
-
- Allon M, Robbin ML: Increasing arteriovenous fistulas in hemodialysis patients: Problems and solutions. Kidney Int 62: 1109–1124, 2002 - PubMed
-
- Ferring M, Henderson J, Wilmink T: Accuracy of early postoperative clinical and ultrasound examination of arteriovenous fistulae to predict dialysis use. J Vasc Access 15: 291–297, 2014 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
