

Cardio-oncology: an overview on outpatient management and future developments
- PMID: 30141030
- PMCID: PMC6220023
- DOI: 10.1007/s12471-018-1148-7
Cardio-oncology: an overview on outpatient management and future developments
Abstract
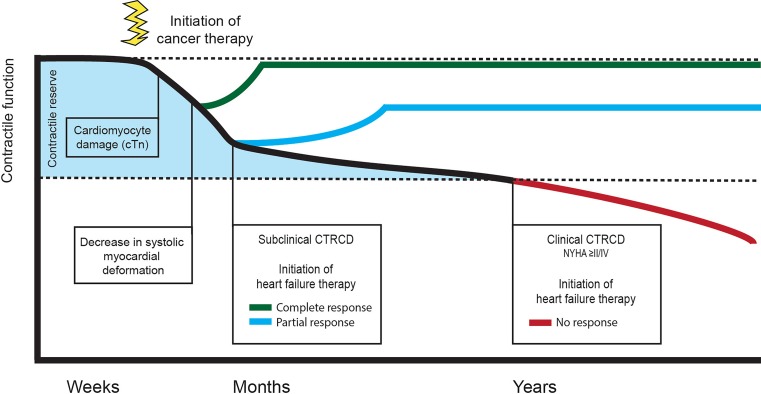
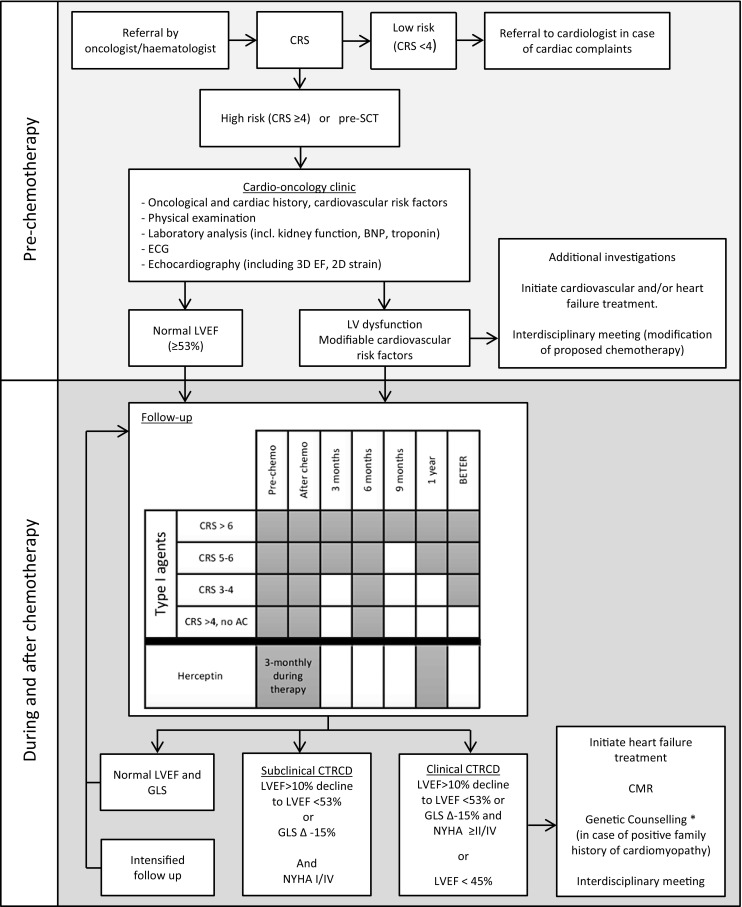
Recent advances in the early detection and treatment of cancer have led to increasing numbers of cancer survivors worldwide. Nonetheless, despite major improvements in the outcome of these patients, long-term side effects of radio- and chemotherapy affect both patient survival and quality of life, independent of the oncological prognosis. Chemotherapy-related cardiac dysfunction is one of the most notorious short-term side effects of anticancer treatment, occurring in ~10% of patients. Progression to overt heart failure carries a strikingly poor prognosis with a 2-year mortality rate of 60%. Early detection of left ventricular damage by periodic monitoring and prompt initiation of heart failure treatment is key in improving cardiovascular prognosis. To meet the growing demand for a specialised interdisciplinary approach for the prevention and management of cardiovascular complications induced by cancer treatment, a new discipline termed cardio-oncology has evolved. However, an uniform, multidisciplinary approach is currently lacking in the Netherlands. This overview provides an introduction and comprehensive summary of this emerging discipline and offers a practical strategy for the outpatient management of this specific patient population.
Keywords: Cardio-oncology; Cardiotoxicity; Chemotherapy; Heart failure.
Conflict of interest statement
A.J. Teske, M. Linschoten, J.A.M. Kamphuis, W.R. Naaktgeboren, T. Leiner, E. van der Wall, J. Kuball, A. van Rhenen, P.A. Doevendans, M.J. Cramer and F.W. Asselbergs declare that they have no competing interests.
Figures
References
-
- Cardinale D. A new frontier: cardio-oncology. Cardiologia. 1996;41:887–891. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
