

Locating the ulnar nerve during elbow arthroscopy using palpation is only accurate proximal to the medial epicondyle
- PMID: 30141147
- PMCID: PMC6754351
- DOI: 10.1007/s00167-018-5108-y
Locating the ulnar nerve during elbow arthroscopy using palpation is only accurate proximal to the medial epicondyle
Abstract
Purpose: Knowledge of ulnar nerve position is of utmost importance to avoid iatrogenic injury in elbow arthroscopy. The aim of this study was to determine how accurate surgeons are in locating the ulnar nerve after fluid extravasation has already occurred, and basing their localization solely on palpation of anatomical landmarks.
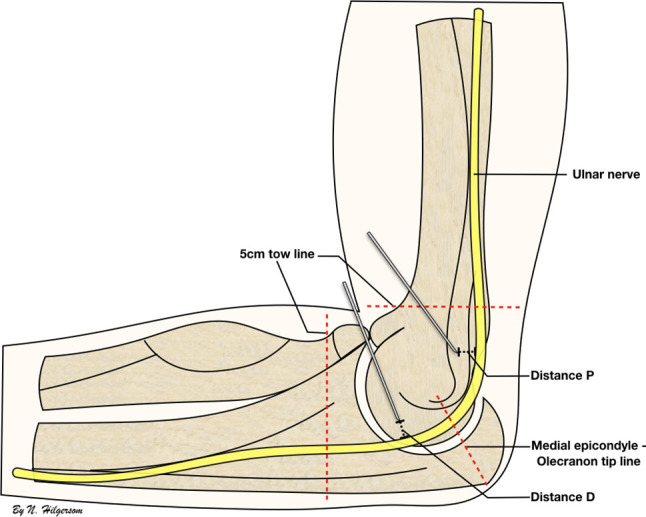
Methods: Seven cadaveric elbows were used and seven experienced surgeons in elbow arthroscopy participated. An arthroscopic setting was simulated and fluids were pumped into the joint from the posterior compartment for 15 min. For each cadaveric elbow, one surgeon was asked to locate the ulnar nerve solely by palpation of the anatomical landmarks, and subsequently pin the ulnar nerve at two positions: within 5 cm proximal and another within 5 cm distal of a line connecting the medial epicondyle and the tip of the olecranon. Subsequently, the elbows were dissected using a standard medial elbow approach and the distances between the pins and ulnar nerve were measured.
Results: The median distance between the ulnar nerve and the proximal pins was 0 mm (range 0-0 mm), and between the ulnar nerve and the distal pins was 2 mm (range 0-10 mm), showing a statistically significant difference (p = 0.009). All seven proximally placed pins (100%) transfixed the ulnar nerve versus two out of seven distally placed pins (29%) (p = 0.021).
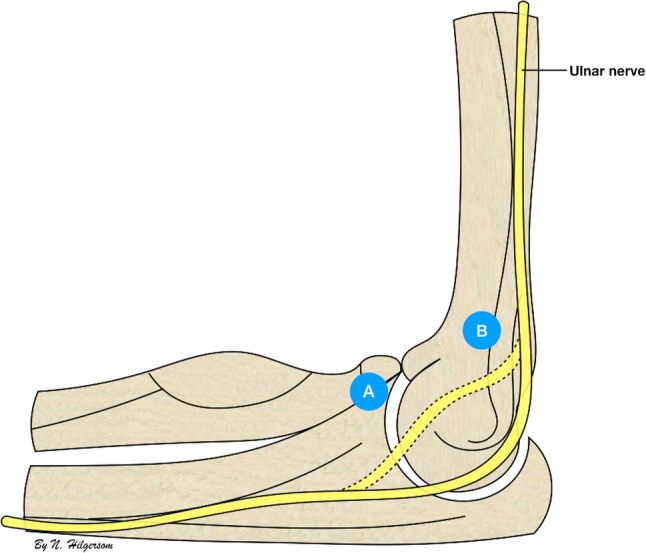
Conclusions: In a setting simulating an already initiated arthroscopic procedure, the sole palpation of the anatomical landmarks allows experienced elbow surgeons to accurately locate the ulnar nerve only in its course proximal to the medial epicondyle (7/7, 100%), whereas a significantly reduced accuracy is documented when the same surgeons attempt to locate the nerve distal to the medial epicondyle (2/7, 29%; p = 0.021). Current findings support the establishment of a proximal anteromedial portal over a distal anteromedial portal to access the anterior compartment after tissue extravasation has occurred with regard to ulnar nerve safety.
Keywords: Arthroscopy; Complication; Elbow; Nerve injury; Physical examination; Prevention; Ulnar nerve.
Conflict of interest statement
The authors, their immediate relatives, and any research foundations with which they are affiliated have not received any financial payments or other benefits from any commercial entity related to the subject of this article.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
