

Predictors of long-term mortality with cardiac resynchronization therapy in mild heart failure patients with left bundle branch block
- PMID: 30141210
- PMCID: PMC6490024
- DOI: 10.1002/clc.23058
Predictors of long-term mortality with cardiac resynchronization therapy in mild heart failure patients with left bundle branch block
Abstract
Background: Cardiac resynchronization therapy (CRT) is highly beneficial in patients with heart failure (HF) and left bundle branch block (LBBB); however, up to 30% of patients in this selected group are nonresponders.
Hypothesis: We hypothesized that clinical and echocardiographic variables can be used to develop a simple mortality risk stratification score in CRT.
Methods: Best-subsets proportional-hazards regression analysis was used to develop a simple clinical risk score for all-cause mortality in 756 patients with LBBB allocated to the CRT with defibrillator (CRT-D) group enrolled in the multicenter automatic defibrillator implantation trial with cardiac resynchronization therapy. The score was used to assess the mortality risk within the CRT-D group and the associations with mortality reduction with CRT-D vs implantable cardioverter defibrillator (ICD) in each risk category.
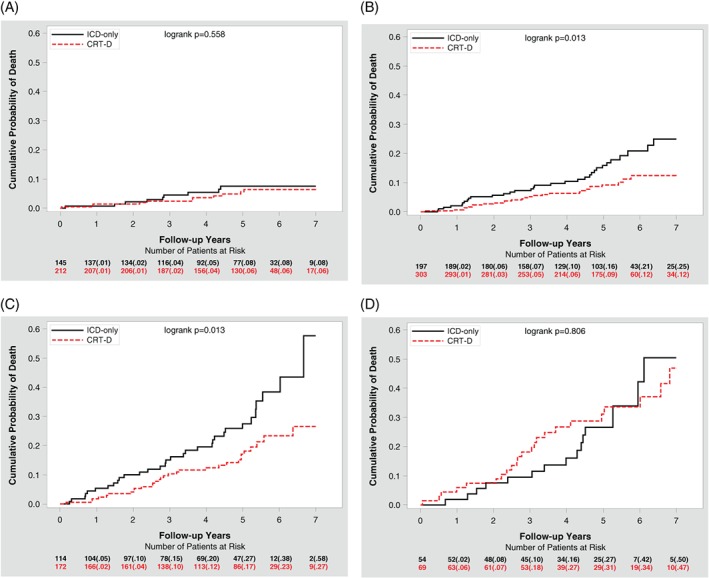
Results: Four clinical variables comprised the risk score: age ≥ 65, creatinine ≥ 1.4 mg/dL, history of coronary artery bypass graft, and left ventricular ejection fraction (LVEF) < 26%. Every 1 point increase in the score was associated with 2-fold increased mortality within the CRT-D arm (P < 0.001). CRT-D was associated with mortality reduction as compared with ICD only in patients with moderate risk: score 0 (HR = 0.80, P = 0.615), score 1 (HR = 0.54, P = 0.019), score 2 (HR = 0.54, P = 0.016), score 3-4 risk factors (HR = 1.08, P = 0.811); however, the device by score interaction was not significant (P = 0.306). The score was also significantly predictive of left ventricular reverse remodeling (P < 0.001).
Conclusions: Four clinical variables can be used for improved mortality risk stratification in mild HF patients with LBBB implanted with CRT-D.
Keywords: cardiac resynchronization therapy; heart failure; left bundle branch block; risk factors.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
Dr Yitschak Biton is a Mirowski‐Moss Career Development Awardee. Drs Ilan Goldenberg, Valentina Kutyifa, and Scott Solomon are receiving grant support from Boston Scientific. No other potential conflict of interest relevant to this article is reported.
Figures

Similar articles
-
Sex Differences in Long-Term Outcomes With Cardiac Resynchronization Therapy in Mild Heart Failure Patients With Left Bundle Branch Block.J Am Heart Assoc. 2015 Jun 29;4(7):e002013. doi: 10.1161/JAHA.115.002013. J Am Heart Assoc. 2015. PMID: 26124205 Free PMC article. Clinical Trial.
-
Differing effects of cardiac resynchronization therapy on long-term mortality in patient subgroups of MADIT-CRT defined by baseline conduction and 1-year post-treatment left ventricular remodeling.Heart Rhythm. 2013 Mar;10(3):366-73. doi: 10.1016/j.hrthm.2012.11.020. Epub 2012 Nov 24. Heart Rhythm. 2013. PMID: 23183194 Clinical Trial.
-
PR interval identifies clinical response in patients with non-left bundle branch block: a Multicenter Automatic Defibrillator Implantation Trial-Cardiac Resynchronization Therapy substudy.Circ Arrhythm Electrophysiol. 2014 Aug;7(4):645-51. doi: 10.1161/CIRCEP.113.001299. Epub 2014 Jun 24. Circ Arrhythm Electrophysiol. 2014. PMID: 24963007 Clinical Trial.
-
Opportunity to increase life span in narrow QRS cardiac resynchronization therapy recipients by deactivating ventricular pacing: evidence from randomized controlled trials.JACC Heart Fail. 2015 Apr;3(4):327-36. doi: 10.1016/j.jchf.2014.11.007. Epub 2015 Mar 11. JACC Heart Fail. 2015. PMID: 25770400 Review.
-
An individual patient meta-analysis of five randomized trials assessing the effects of cardiac resynchronization therapy on morbidity and mortality in patients with symptomatic heart failure.Eur Heart J. 2013 Dec;34(46):3547-56. doi: 10.1093/eurheartj/eht290. Epub 2013 Jul 29. Eur Heart J. 2013. PMID: 23900696 Free PMC article. Review.
Cited by
-
Risk scores in cardiac resynchronization therapy-A review of the literature.Front Cardiovasc Med. 2023 Jan 17;9:1048673. doi: 10.3389/fcvm.2022.1048673. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36733831 Free PMC article. Review.
-
Response to cardiac resynchronization therapy in non-ischemic cardiomyopathy is unrelated to medical therapy.Clin Cardiol. 2019 Jan;42(1):143-150. doi: 10.1002/clc.23123. Epub 2018 Dec 15. Clin Cardiol. 2019. PMID: 30467886 Free PMC article.
References
-
- Linde C, Abraham WT, Gold MR, et al. REVERSE (REsynchronization reVErses Remodeling in Systolic left vEntricular dysfunction) Study Group. Randomized trial of cardiac resynchronization in mildly symptomatic heart failure patients and in asymptomatic patients with left ventricular dysfunction and previous heart failure symptoms. J Am Coll Cardiol. 2008;52:1834‐1843. - PubMed
-
- Bristow MR, Saxon LA, Boehmer J, et al. Comparison of Medical Therapy, Pacing, and Defibrillation in Heart Failure (COMPANION) Investigators. Cardiac‐resynchronization therapy with or without an implantable defibrillator in advanced chronic heart failure. N Engl J Med. 2004;350:2140‐2150. - PubMed
-
- Cleland JG, Daubert J‐C, Erdmann E, et al. Cardiac Resynchronization‐Heart Failure (CARE‐HF) Study Investigators. The effect of cardiac resynchronization on morbidity and mortality in heart failure. N Engl J Med. 2005;352:1539‐1549. - PubMed
-
- Goldenberg I, Kutyifa V, Klein HU, et al. Survival with cardiac‐resynchronization therapy in mild heart failure. N Engl J Med. 2014;370:1694‐1701. - PubMed
-
- Moss AJ, Hall WJ, Cannom DS, et al. MADIT‐CRT Trial Investigators. Cardiac‐resynchronization therapy for the prevention of heart‐failure events. N Engl J Med. 2009;361:1329‐1338. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
