

Comparison of robot-assisted surgery, laparoscopic-assisted surgery, and open surgery for the treatment of colorectal cancer: A network meta-analysis
- PMID: 30142771
- PMCID: PMC6112974
- DOI: 10.1097/MD.0000000000011817
Comparison of robot-assisted surgery, laparoscopic-assisted surgery, and open surgery for the treatment of colorectal cancer: A network meta-analysis
Abstract
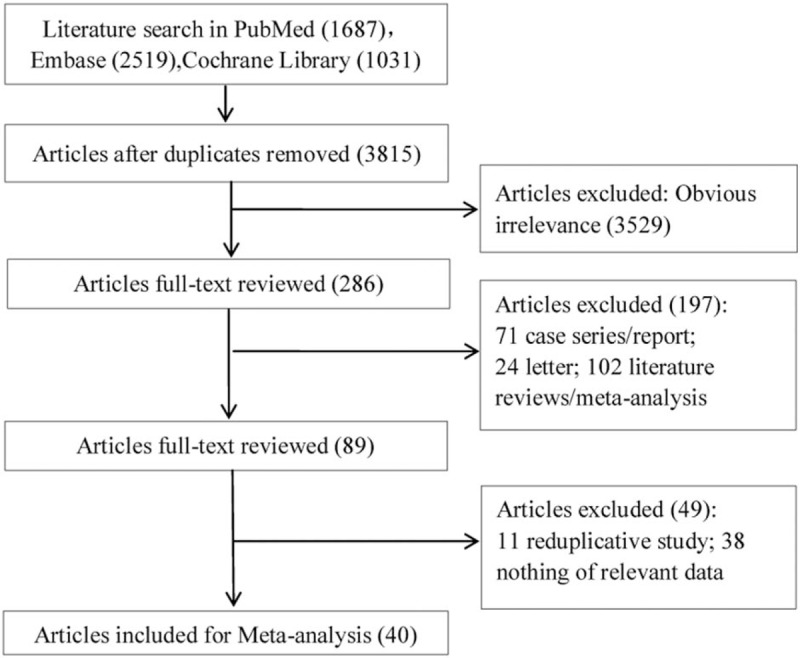
Background: The aim of this study was to find the better treatment for colorectal cancer (CRC) by comparing robot-assisted colorectal surgery (RACS), laparoscopic-assisted colorectal surgery (LACS), and open surgery using network meta-analysis.
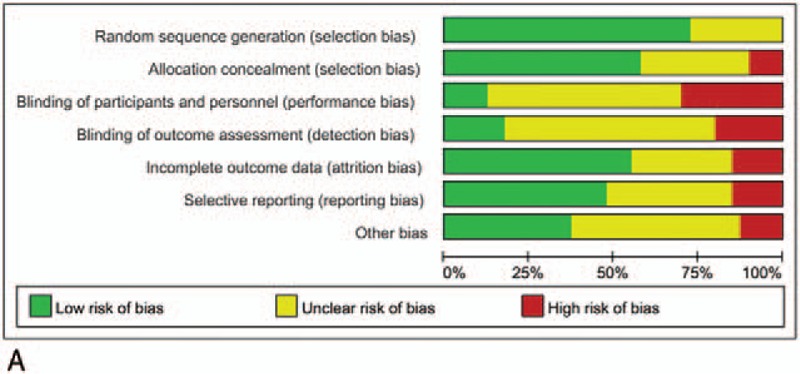
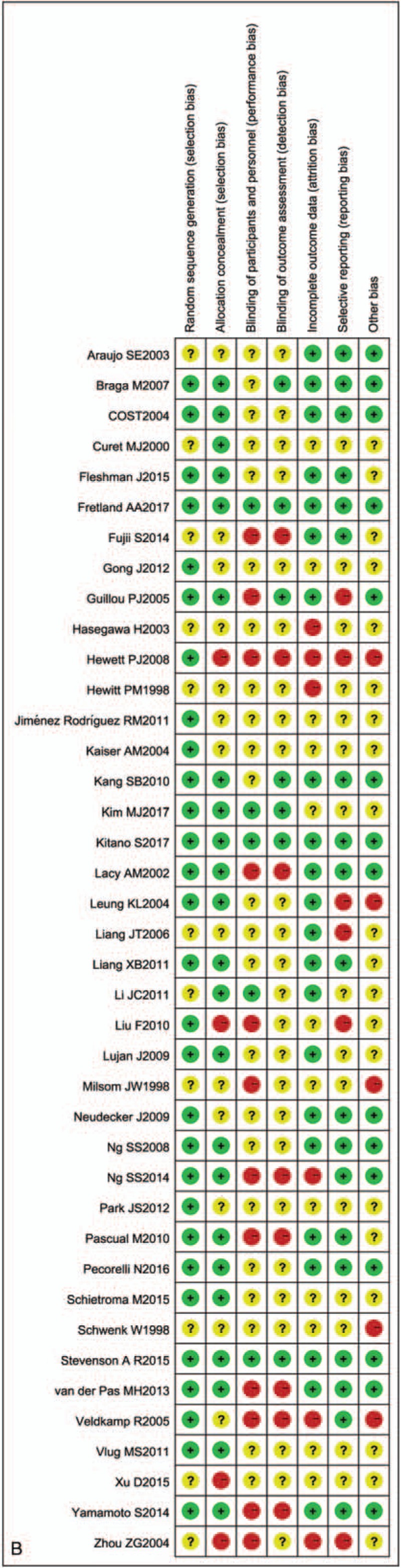
Methods: A literature search updated to August 15, 2017 was performed. All the included literatures were evaluated according to the quality evaluation criteria of bias risk recommended by the Cochrane Collaboration. All data were comprehensively analyzed by ADDIS. Odds ratio (OR), mean difference (MD), and 95% confidence interval (CI) were used to show the effect index of all data. The degree of convergence of the model was evaluated by the Brooks-Gelman-Rubin method with the potential scale reduction factor (PSRF) as the evaluation indicator.
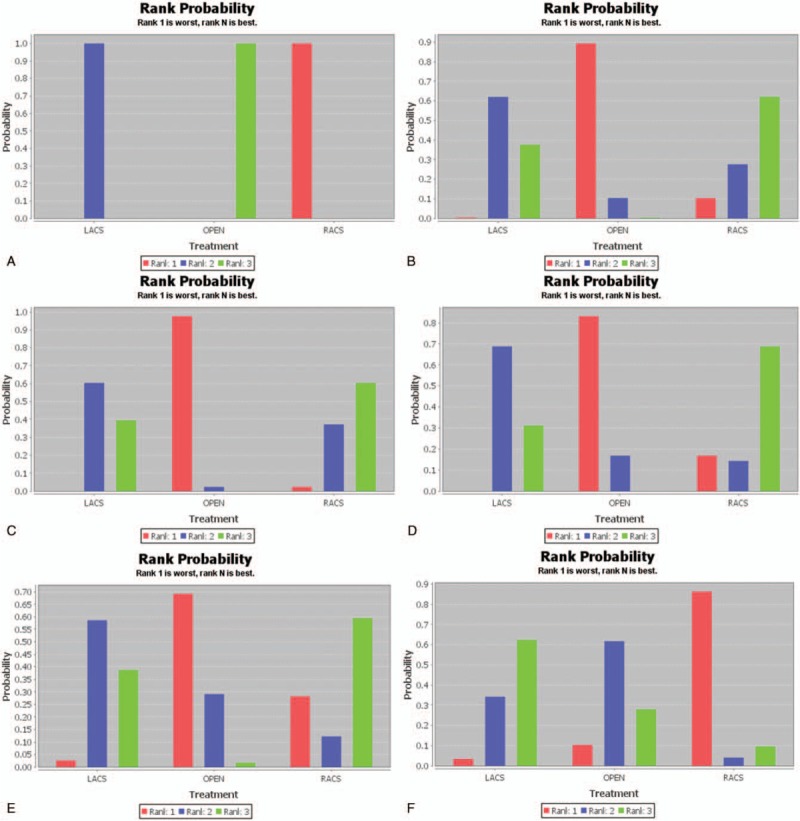
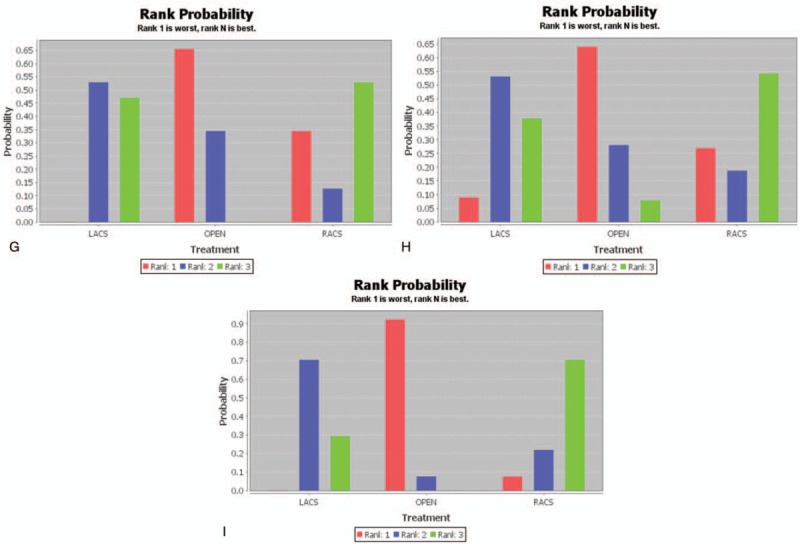
Results: The PSRF values of operation time, estimated blood loss, length of hospital stay, complication, mortality, and anastomotic leakage ranged from 1.00 to 1.01, and those of wound infection, bleeding, and ileus ranged from 1.00 to 1.02. Open surgery had the shortest operation time compared with LACS and RACS. Furthermore, compared with LACS, the amount of blood loss, complication, mortality, bleeding rate, and ileus rate for RACS were the least, and the length of hospital stay for RACS was the shortest. The anastomotic leakage rate for LACS was the least, but there was no significant difference compared with those of RACS and open surgery. The wound infection rate for LACS was the least, but there was no significant difference compared with that of RACS.
Conclusion: RACS might be a better treatment for patients with CRC.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Siegel RL, Miller KD, Fedewa SA, et al. Colorectal cancer statistics, 2017. CA Cancer J Clin 2017;67:177. - PubMed
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015;65:87. - PubMed
-
- Battaglia RE, Baumer B, Conrad B, et al. Health risks associated with meat consumption: a review of epidemiological studies. Int J Vit Nutr Res 2015;85:70. - PubMed
-
- Blase JL, Campbell PT, Gapstur SM, et al. Prediagnostic Helicobacter pylori antibodies and colorectal cancer risk in an elderly, Caucasian population. Helicobacter 2016;21:488–92. - PubMed
-
- De RK, De BM, Huybrechts I, et al. Dietary mycotoxins, co-exposure, and carcinogenesis in humans: short review. Mutat Res Rev Mutat Res 2015;766:32. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
