

External validation of computed tomography decision rules for minor head injury: prospective, multicentre cohort study in the Netherlands
- PMID: 30143521
- PMCID: PMC6108278
- DOI: 10.1136/bmj.k3527
External validation of computed tomography decision rules for minor head injury: prospective, multicentre cohort study in the Netherlands
Abstract
Objective: To externally validate four commonly used rules in computed tomography (CT) for minor head injury.
Design: Prospective, multicentre cohort study.
Setting: Three university and six non-university hospitals in the Netherlands.
Participants: Consecutive adult patients aged 16 years and over who presented with minor head injury at the emergency department with a Glasgow coma scale score of 13-15 between March 2015 and December 2016.
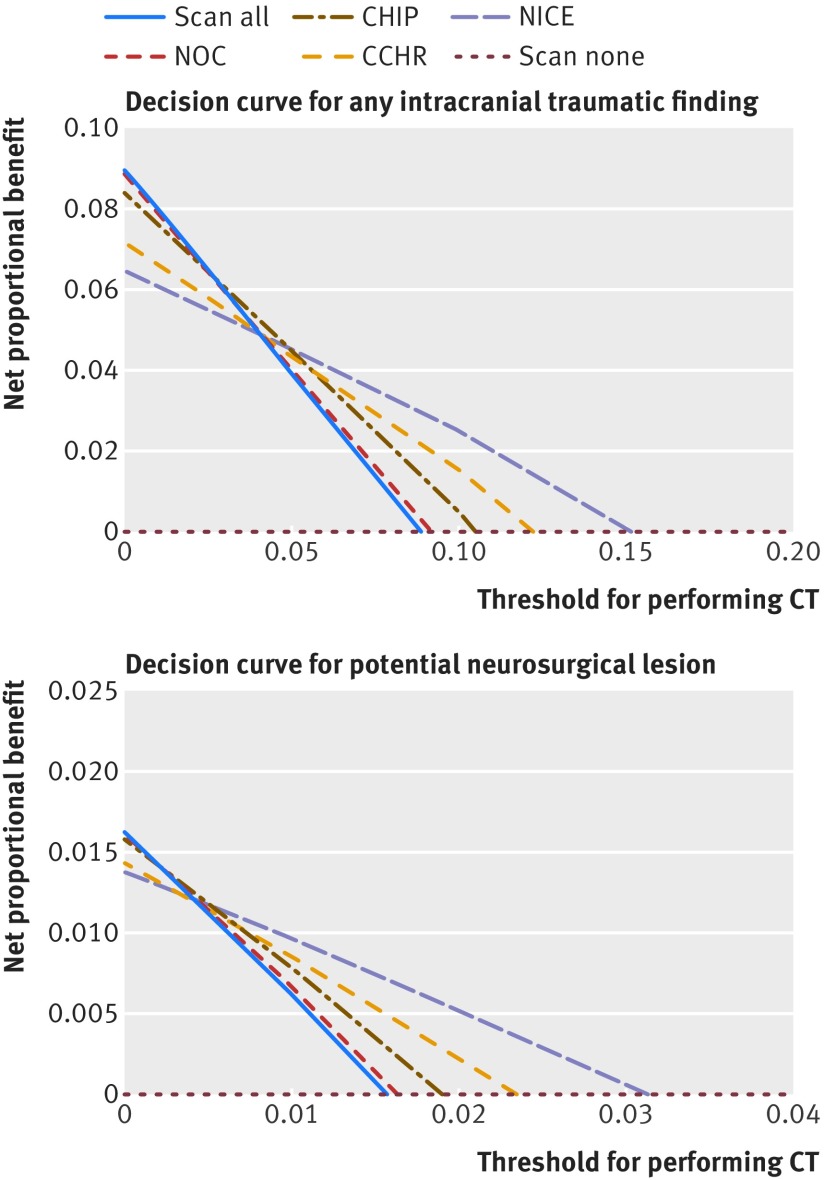
Main outcome measures: The primary outcome was any intracranial traumatic finding on CT; the secondary outcome was a potential neurosurgical lesion on CT, which was defined as an intracranial traumatic finding on CT that could lead to a neurosurgical intervention or death. The sensitivity, specificity, and clinical usefulness (defined as net proportional benefit, a weighted sum of true positive classifications) of the four CT decision rules. The rules included the CT in head injury patients (CHIP) rule, New Orleans criteria (NOC), Canadian CT head rule (CCHR), and National Institute for Health and Care Excellence (NICE) guideline for head injury.
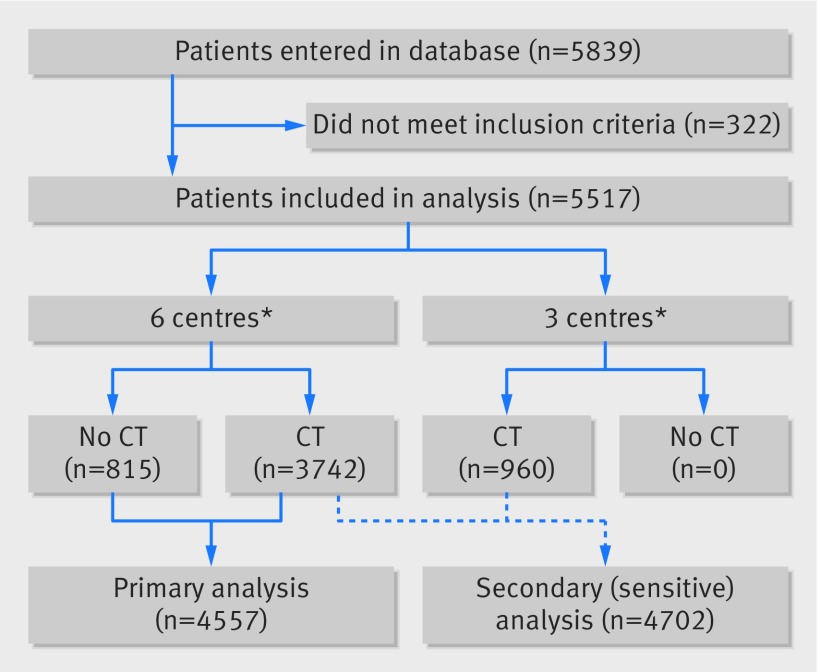
Results: For the primary analysis, only six centres that included patients with and without CT were selected. Of 4557 eligible patients who presented with minor head injury, 3742 (82%) received a CT scan; 384 (8%) had a intracranial traumatic finding on CT, and 74 (2%) had a potential neurosurgical lesion. The sensitivity for any intracranial traumatic finding on CT ranged from 73% (NICE) to 99% (NOC); specificity ranged from 4% (NOC) to 61% (NICE). Sensitivity for a potential neurosurgical lesion ranged between 85% (NICE) and 100% (NOC); specificity from 4% (NOC) to 59% (NICE). Clinical usefulness depended on thresholds for performing CT scanning: the NOC rule was preferable at a low threshold, the NICE rule was preferable at a higher threshold, whereas the CHIP rule was preferable for an intermediate threshold.
Conclusions: Application of the CHIP, NOC, CCHR, or NICE decision rules can lead to a wide variation in CT scanning among patients with minor head injury, resulting in many unnecessary CT scans and some missed intracranial traumatic findings. Until an existing decision rule has been updated, any of the four rules can be used for patients presenting minor head injuries at the emergency department. Use of the CHIP rule is recommended because it leads to a substantial reduction in CT scans while missing few potential neurosurgical lesions.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no specific support from any organisation for the submitted work; MGMH and DWJD were the principal investigators of the CHIP (CT in head injury patients) development study; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
Comment in
-
In minor head trauma, decision rules were sensitive for intracranial findings, but reductions in CT use varied.Ann Intern Med. 2018 Dec 18;169(12):JC71. doi: 10.7326/ACPJC-2018-169-12-071. Ann Intern Med. 2018. PMID: 30557424 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical