

Making HPV vaccination available to girls everywhere
- PMID: 30144050
- PMCID: PMC6221992
- DOI: 10.1002/ijgo.12656
Making HPV vaccination available to girls everywhere
Abstract
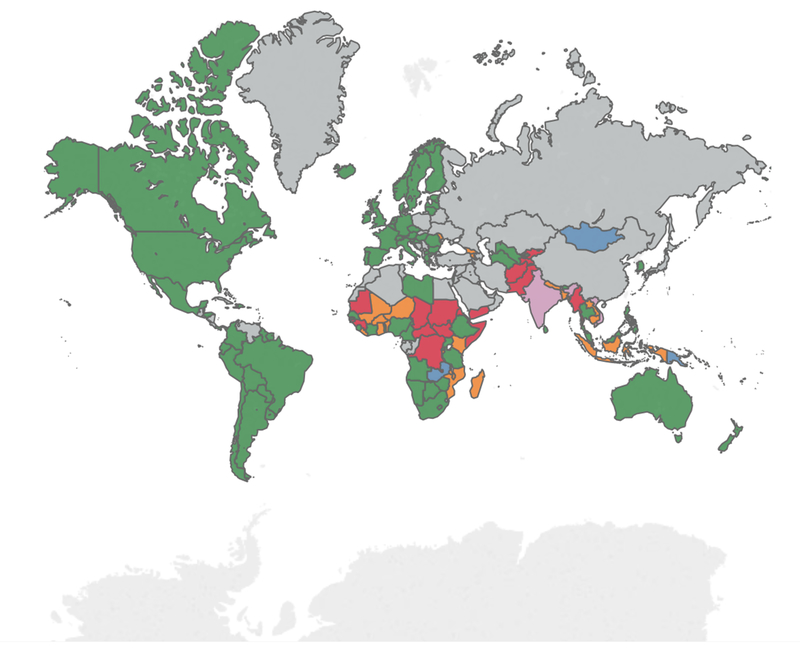
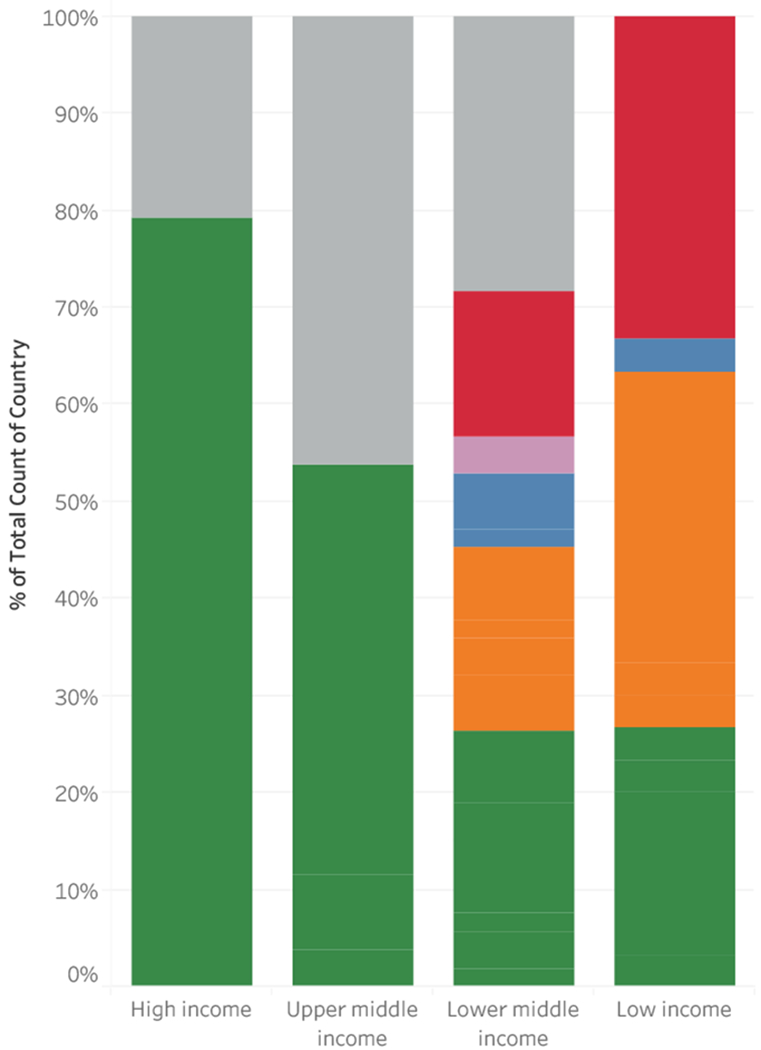
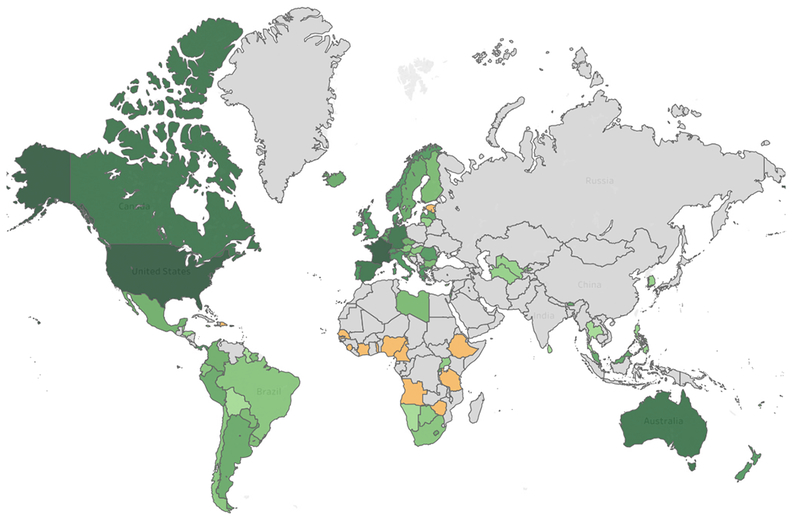
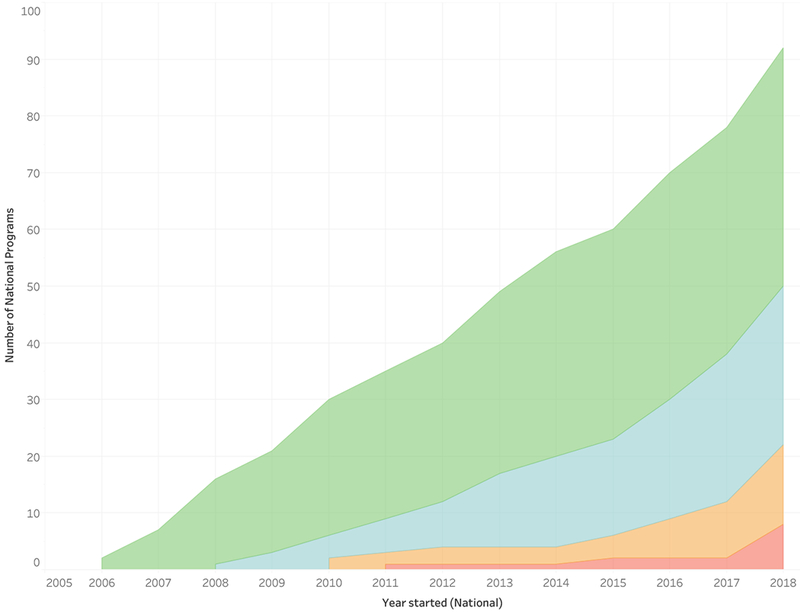
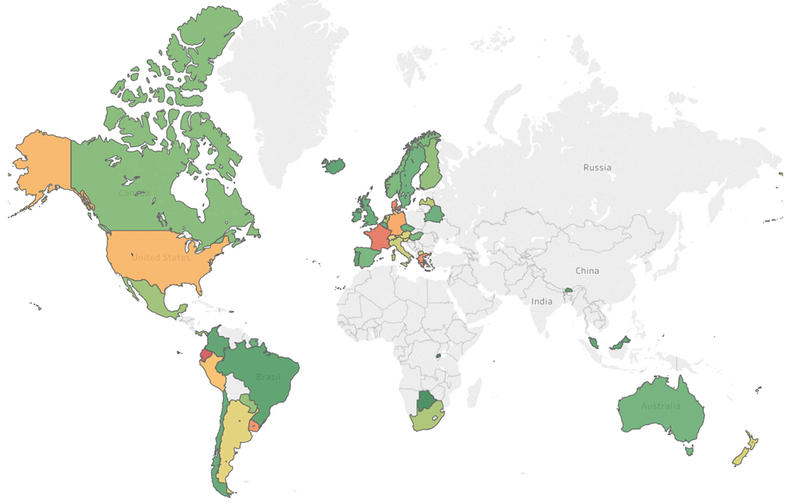
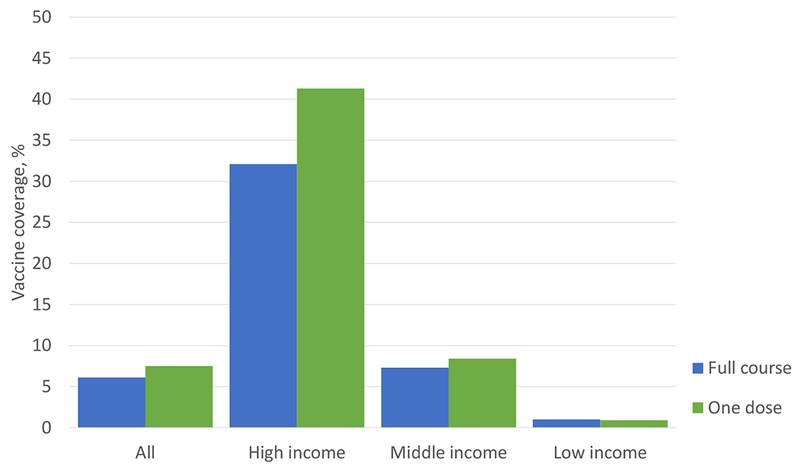
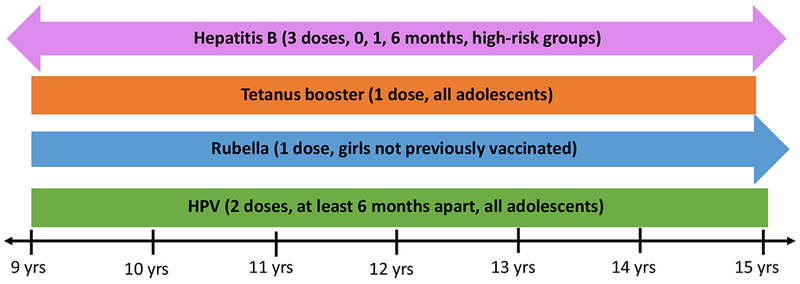
Cervical cancer is currently the fourth leading cause of cancer death among women worldwide, with most cases occurring in low- and middle-income countries. Safe, highly effective vaccines against HPV have been on the market since 2006, yet only 6% of girls worldwide have received this life-saving cancer prevention intervention. International organizations, including PATH, Gavi, and the pharmaceutical companies Merck and GlaxoSmithKline, have provided support to eligible low- and middle-income countries to implement national HPV vaccination programs. Still, glaring disparities in the availability of national HPV vaccination programs and the coverage of the primary target population between the global north and south persist. We illustrate worldwide HPV vaccine implementation and coverage using an online data visualization, which is publicly available and can be used to gain unique insights. We also present three emerging solutions to transform future HPV vaccine delivery in low- and middle-income countries: low-cost generics, single-dose vaccination, and co-administration with other adolescent vaccines. By rapidly expanding access to HPV vaccination to girls everywhere, vaccine-type HPV infections can be virtually eliminated. At high vaccination-coverage levels, more than 80%-or approximately 230 000-of the cervical cancer deaths that occur each year can be averted.
Keywords: Cervical cancer prevention; Co-administration; Coverage; Dosing schedule; Human papillomavirus; Impact; Low- and middle-income countries; Vaccination.
© 2018 International Federation of Gynecology and Obstetrics.
Conflict of interest statement
Conflict of interest
The authors have no conflicts of interest.
Figures
References
-
- Ervik M, Lam F, Ferlay J, Mery L, Soerjomataram I, Bray F. Cancer Today. Lyon, France: International Agency for Research on Cancer; 2016. Available from: http://gco.iarc.fr/today. Accessed May 1, 2017.
-
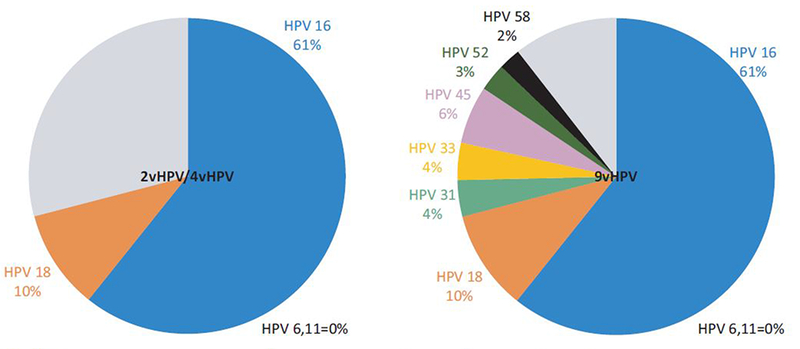
- Serrano B, de Sanjose S, Tous S, et al. Human papillomavirus genotype attribution for HPVs 6, 11, 16, 18, 31, 33, 45, 52 and 58 in female anogenital lesions. Eur J Cancer. 2015;51(13):1732–1741. - PubMed
-
- Cervarix Package Insert. GlaxoSmithKline; 2009.
-
- Gardasil Package Insert. Merck & Co., Inc.; 2011.
-
- Gardasil-9 Package Insert. Merck & Co., Inc.; 2018.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
