

Standard Bronchoscopy With Fluoroscopy vs Thin Bronchoscopy and Radial Endobronchial Ultrasound for Biopsy of Pulmonary Lesions: A Multicenter, Prospective, Randomized Trial
- PMID: 30144421
- PMCID: PMC6224707
- DOI: 10.1016/j.chest.2018.08.1026
Standard Bronchoscopy With Fluoroscopy vs Thin Bronchoscopy and Radial Endobronchial Ultrasound for Biopsy of Pulmonary Lesions: A Multicenter, Prospective, Randomized Trial
Abstract
Background: New technology has resulted in bronchoscopy being increasingly used for diagnosing pulmonary lesions. Reported yield from these procedures varies widely with few randomized clinical trials. This study compares the diagnostic yield of a thin bronchoscope and radial endobronchial ultrasound (R-EBUS) with standard bronchoscopy and fluoroscopy (SB-F) in lung lesions.
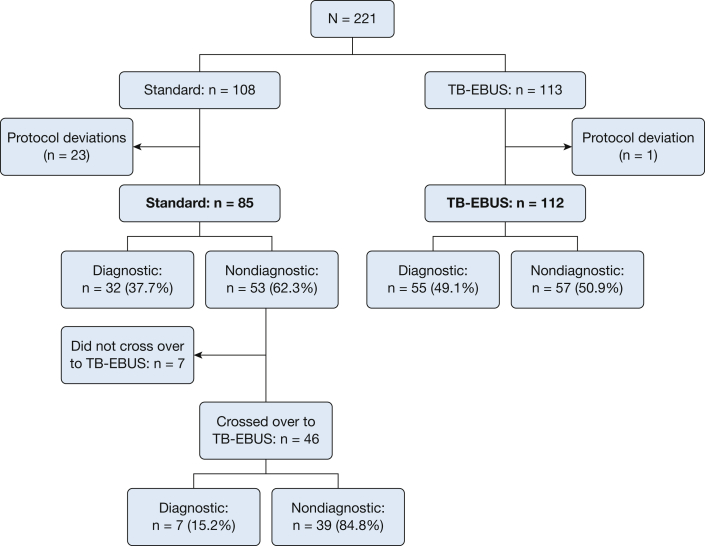
Methods: Patients presenting for diagnostic bronchoscopic evaluation at five centers were randomized to undergo SB-F or R-EBUS with a thin bronchoscope (TB-EBUS). If SB-F was nondiagnostic, crossover to the TB-EBUS arm was allowed. Data on patient demographics, radiographic features, and final pathologic or radiographic follow-up were collected. Statistical comparisons were made by Fisher exact test, χ2 test, and Student t test. Bivariate and multivariate analyses were performed to determine predictors of diagnostic yield.
Results: One hundred and ninety-seven patients were included in the final analyses. There was no difference in demographics, lesion size, or location between study arms. The average lesion size was 31.2 mm (SD, 10.8 mm). Bronchoscopy was diagnostic in 87 patients (44%). Although the diagnostic yield was higher in the TB-EBUS arm compared with the SB-F arm (49% vs 37%), this difference was not statistically significant (P = .11). Among those with nondiagnostic bronchoscopic findings in the standard arm, 87% (n = 46) crossed over to TB-EBUS, resulting in a diagnosis in seven additional patients (15% of 46).
Conclusions: Bronchoscopy with or without a thin scope and R-EBUS had a poor diagnostic yield for pulmonary lesions. Future work should focus on improvements in technique and technology advances that ensure a higher likelihood of obtaining a diagnosis.
Keywords: bronchoscopy; guided bronchoscopy; lung lesion; radial endobronchial ultrasound.
Published by Elsevier Inc.
Figures
References
-
- Rivera M.P., Mehta A.C., Wahidi M.M. Establishing the diagnosis of lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 suppl):e142S–e165S. - PubMed
-
- Gould M.K., Tang T., Liu I.L. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med. 2015;192(10):1208–1214. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
