

Accuracy of Microelectrode Trajectory Adjustments during DBS Assessed by Intraoperative CT
- PMID: 30145596
- PMCID: PMC6214613
- DOI: 10.1159/000489945
Accuracy of Microelectrode Trajectory Adjustments during DBS Assessed by Intraoperative CT
Abstract
Background/aims: Microelectrode recording (MER)-guided deep brain stimulation (DBS) aims to place the DBS lead in the optimal electrophysiological target. When single-track MER or test stimulation yields suboptimal results, trajectory adjustments are made. The accuracy of these trajectory adjustments is unknown. Intraoperative computed tomography can visualize the microelectrode (ME) and verify ME adjustments. We aimed to determine the accuracy of ME movements in patients undergoing MER-guided DBS.
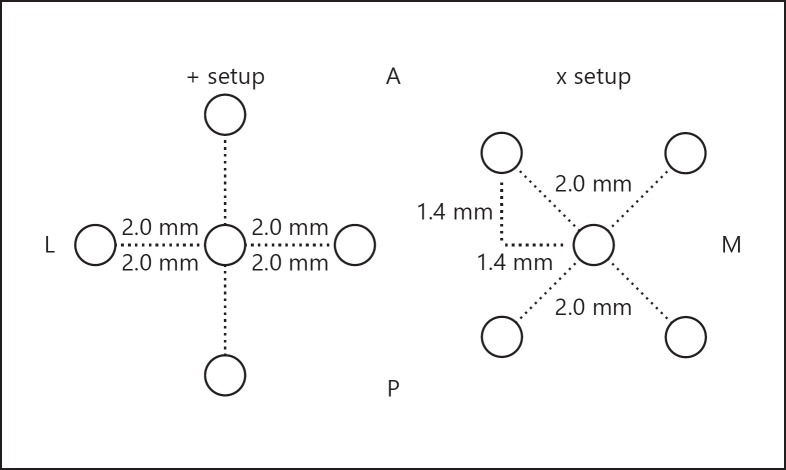
Methods: Coordinates following three methods of adjustment were compared: (1) those within the default "+" configuration of the ME holder; (2) those involving rotation of the default "+" to the "x" configuration; and (3) those involving head stage adjustments. Radial error and absolute differences between coordinates were determined.
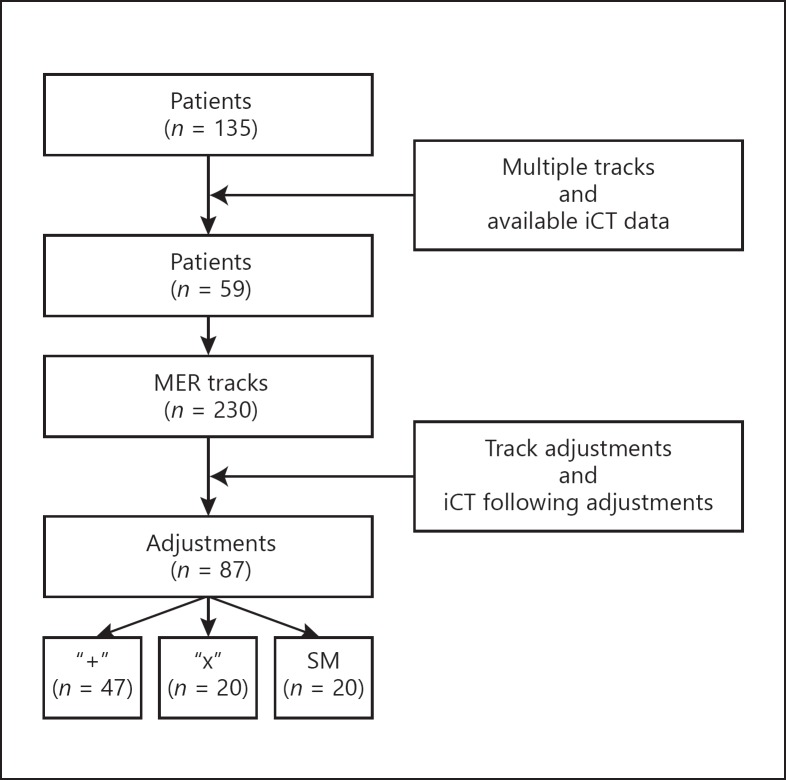
Results: 87 ME movements in 59 patients were analyzed. Median (IQR) radial error was 0.59 (0.64) mm. Median (IQR) absolute x and y coordinate errors were 0.29 (0.52) and 0.38 (0.44) mm, respectively. Errors were largest after rotating the multielectrode holder to its "x"-shaped setup.
Conclusion: ME trajectory adjustments can be made accurately. In a considerable number of cases, errors exceeding 1 mm were found. Adjustments from the "+" setup to the "x" setup are most prone to inaccuracies.
Keywords: Deep brain stimulation; Intraoperative computed tomography; Microelectrode movement; Microelectrode recording.
© 2018 The Author(s) Published by S. Karger AG, Basel.
Figures
References
-
- Deuschl G, Schade-Brittinger C, Krack P, Volkmann J, Schäfer H, Bötzel K, et al. A randomized trial of deep-brain stimulation for Parkinson's disease. N Engl J Med. 2006;355:896–908. - PubMed
-
- Volkmann J, Mueller J, Deuschl G, Kühn AA, Krauss JK, Poewe W, et al. Pallidal neurostimulation in patients with medication-refractory cervical dystonia: a randomised, sham-controlled trial. Lancet Neurol. 2014;13:875–884. - PubMed
-
- Schuurman PR, Bosch DA, Merkus MP, Speelman JD. Long-term follow-up of thalamic stimulation versus thalamotomy for tremor suppression. Mov Disord. 2008;23:1146–1153. - PubMed
-
- Goodman WK, Alterman RL. Deep brain stimulation for intractable psychiatric disorders. Annu Rev Med. 2012;63:511–524. - PubMed
-
- Kennedy SH, Giacobbe P, Rizvi SJ, Placenza FM, Nishikawa Y, Mayberg HS, et al. Deep brain stimulation for treatment-resistant depression: follow-up after 3 to 6 years. Am J Psychiatry. 2011;168:502–510. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
