

Risk of ESRD and Mortality in Kidney and Bladder Stone Formers
- PMID: 30146423
- PMCID: PMC6252145
- DOI: 10.1053/j.ajkd.2018.06.012
Risk of ESRD and Mortality in Kidney and Bladder Stone Formers
Abstract
Rationale & objectives: Kidney stones have been associated with increased risk for end-stage renal disease (ESRD). However, it is unclear whether there is also an increased risk for mortality and if these risks are uniform across clinically distinct categories of stone formers.
Study design: Historical matched-cohort study.
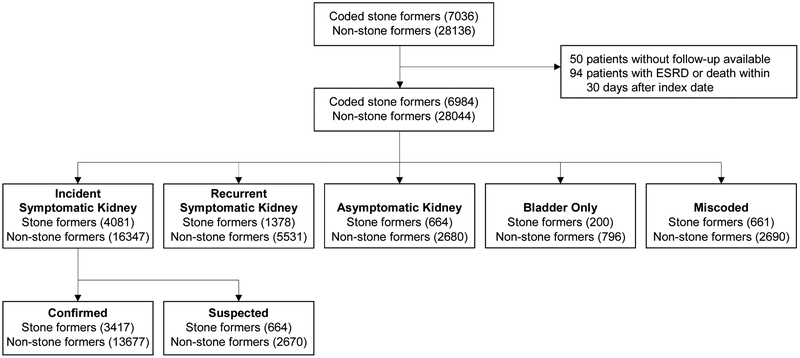
Setting & participants: Stone formers in Olmsted County, MN, between 1984 and 2012 identified using International Classification of Diseases, Ninth Revision codes. Age- and sex-matched individuals who had no codes for stones were the comparison group.
Predictor: Stone formers were placed into 5 mutually exclusive categories after review of medical charts: incident symptomatic kidney, recurrent symptomatic kidney, asymptomatic kidney, bladder only, and miscoded (no stone).
Outcomes: ESRD, mortality, cardiovascular mortality, and cancer mortality.
Analytical approach: Cox proportional hazards models with adjustment for baseline comorbid conditions.
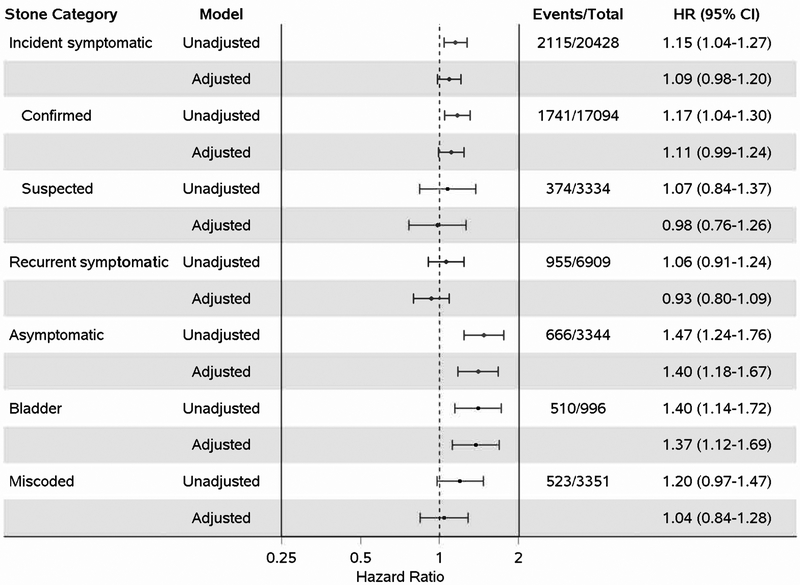
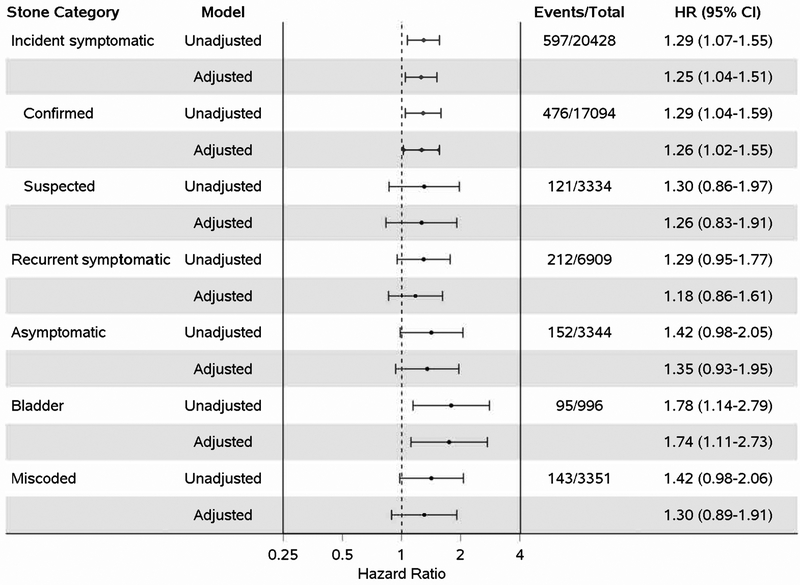
Results: Overall, 65 of 6,984 (0.93%) stone formers and 102 of 28,044 (0.36%) non-stone formers developed ESRD over a mean follow-up of 12.0 years. After adjusting for baseline hypertension, diabetes mellitus, dyslipidemia, gout, obesity, and chronic kidney disease, risk for ESRD was higher in recurrent symptomatic kidney (HR, 2.34; 95% CI, 1.08-5.07), asymptomatic kidney (HR, 3.94; 95% CI, 1.65-9.43), and miscoded (HR, 6.18; 95% CI, 2.25-16.93) stone formers, but not in incident symptomatic kidney or bladder stone formers. The adjusted risk for all-cause mortality was higher in asymptomatic kidney (HR, 1.40; 95% CI, 1.18-1.67) and bladder (HR, 1.37; 95% CI, 1.12-1.69) stone formers. Chart review of asymptomatic and miscoded stone formers suggested increased risk for adverse outcomes related to diagnoses including urinary tract infection, cancer, and musculoskeletal or gastrointestinal pain.
Conclusions: The higher risk for ESRD in recurrent symptomatic compared with incident symptomatic kidney stone formers suggests that stone events are associated with kidney injury. The clinical indication for imaging in asymptomatic stone formers, the correct diagnosis in miscoded stone formers, and the cause of a bladder outlet obstruction in bladder stone formers may explain the higher risk for ESRD or death in these groups.
Keywords: Kidney stones; all-cause mortality; bladder stones; cancer mortality; cardiovascular mortality; chronic kidney disease (CKD); end-stage renal disease (ESRD); kidney disease risk factor; nephrolithiasis; recurrent stone formation.
Copyright © 2018 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
Long-term Adverse Outcomes of Urolithiasis.Am J Kidney Dis. 2018 Dec;72(6):774-775. doi: 10.1053/j.ajkd.2018.07.021. Am J Kidney Dis. 2018. PMID: 30470296 No abstract available.
References
-
- Zhe M, Hang Z. Nephrolithiasis as a risk factor of chronic kidney disease: a meta-analysis of cohort studies with 4,770,691 participants. Urolithiasis. 2017;45(5):441–448. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
