

Profile of intravenous glyburide for the prevention of cerebral edema following large hemispheric infarction: evidence to date
- PMID: 30147301
- PMCID: PMC6101021
- DOI: 10.2147/DDDT.S150043
Profile of intravenous glyburide for the prevention of cerebral edema following large hemispheric infarction: evidence to date
Abstract
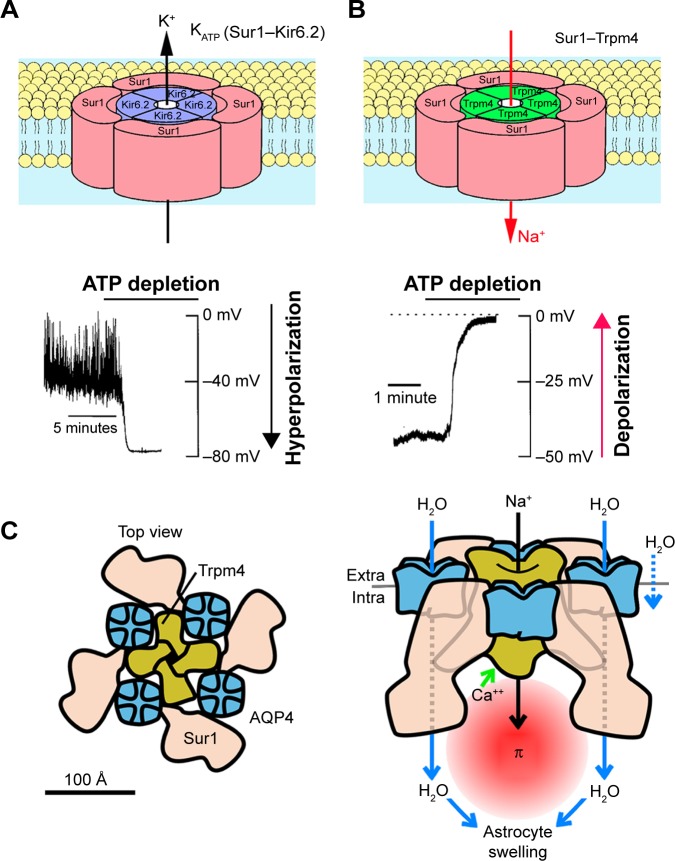
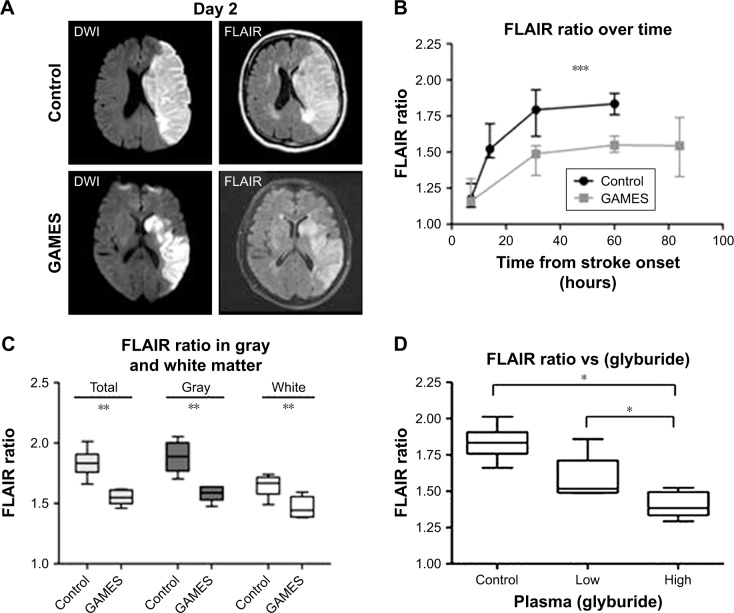
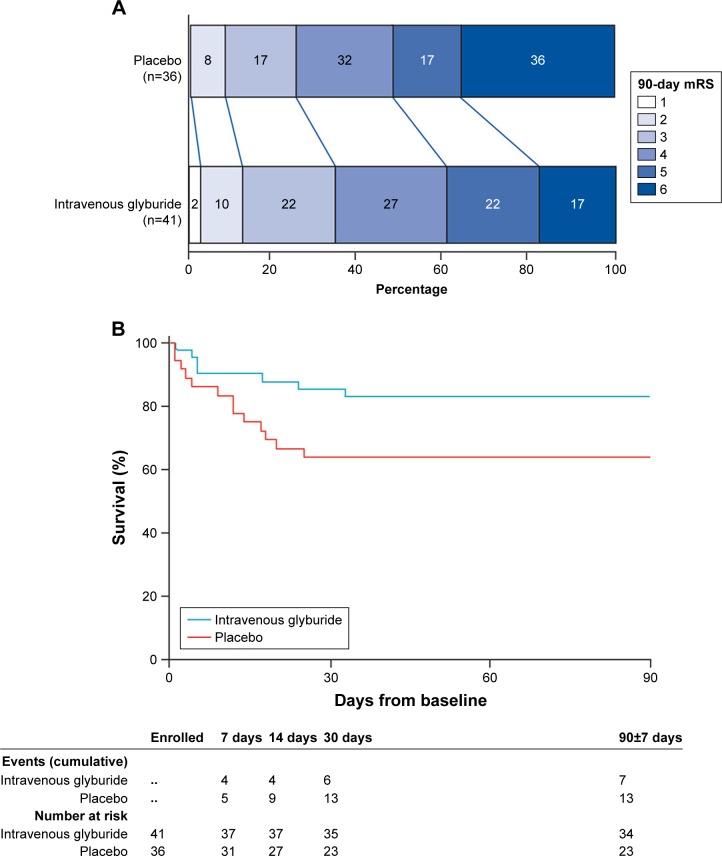
Glyburide (also known as glibenclamide) is a second-generation sulfonylurea drug that inhibits sulfonylurea receptor 1 (Sur1) at nanomolar concentrations. Long used to target KATP (Sur1-Kir6.2) channels for the treatment of diabetes mellitus type 2, glyburide was recently repurposed to target Sur1-transient receptor potential melastatin 4 (Trpm4) channels in acute central nervous system injury. Discovered nearly two decades ago, SUR1-TRPM4 has emerged as a critical target in stroke, specifically in large hemispheric infarction, which is characterized by edema formation and life-threatening brain swelling. Following ischemia, SUR1-TRPM4 channels are transcriptionally upregulated in all cells of the neurovascular unit, including neurons, astrocytes, microglia, oligodendrocytes and microvascular endothelial cells. Work by several independent laboratories has linked SUR1-TRPM4 to edema formation, with blockade by glyburide reducing brain swelling and death in preclinical models. Recent work showed that, following ischemia, SUR1-TRPM4 co-assembles with aquaporin-4 to mediate cellular swelling of astrocytes, which contributes to brain swelling. Additionally, recent work linked SUR1-TRPM4 to secretion of matrix metalloproteinase-9 (MMP-9) induced by recombinant tissue plasminogen activator in activated brain endothelial cells, with blockade of SUR1-TRPM4 by glyburide reducing MMP-9 and hemorrhagic transformation in preclinical models with recombinant tissue plasminogen activator. The recently completed GAMES (Glyburide Advantage in Malignant Edema and Stroke) clinical trials on patients with large hemispheric infarctions treated with intravenous glyburide (RP-1127) revealed promising findings with regard to brain swelling (midline shift), MMP-9, functional outcomes and mortality. Here, we review key elements of the basic science, preclinical experiments and clinical studies, both retrospective and prospective, on glyburide in focal cerebral ischemia and stroke.
Keywords: brain swelling; cerebral ischemia; glyburide; malignant edema; matrix metalloproteinase-9; stroke; sulfonylurea receptor 1.
Conflict of interest statement
Disclosure JMS holds a US patent (7,285,574), “A novel non-selective cation channel in neural cells and methods for treating brain swelling.” JMS is a member of the Board of Directors and holds shares in Remedy Pharmaceuticals, and is a paid consultant for Biogen. No support, direct or indirect, was provided to JMS, or for this project, by Remedy Pharmaceuticals or by Biogen. The authors report no other conflicts of interest in this work.
Figures
References
-
- Hacke W, Schwab S, Horn M, Spranger M, de Georgia M, von Kummer R, von KR. ‘Malignant’ middle cerebral artery territory infarction: clinical course and prognostic signs. Arch Neurol. 1996;53(4):309–315. - PubMed
-
- Berrouschot J, Sterker M, Bettin S, Köster J, Schneider D. Mortality of space-occupying (‘malignant’) middle cerebral artery infarction under conservative intensive care. Intensive Care Med. 1998;24(6):620–623. - PubMed
-
- Kleindorfer D, Lindsell CJ, Brass L, Koroshetz W, Broderick JP. National US estimates of recombinant tissue plasminogen activator use: ICD-9 codes substantially underestimate. Stroke. 2008;39(3):924–928. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
