

The Lung in Primary Immunodeficiencies: New Concepts in Infection and Inflammation
- PMID: 30147696
- PMCID: PMC6096054
- DOI: 10.3389/fimmu.2018.01837
The Lung in Primary Immunodeficiencies: New Concepts in Infection and Inflammation
Abstract
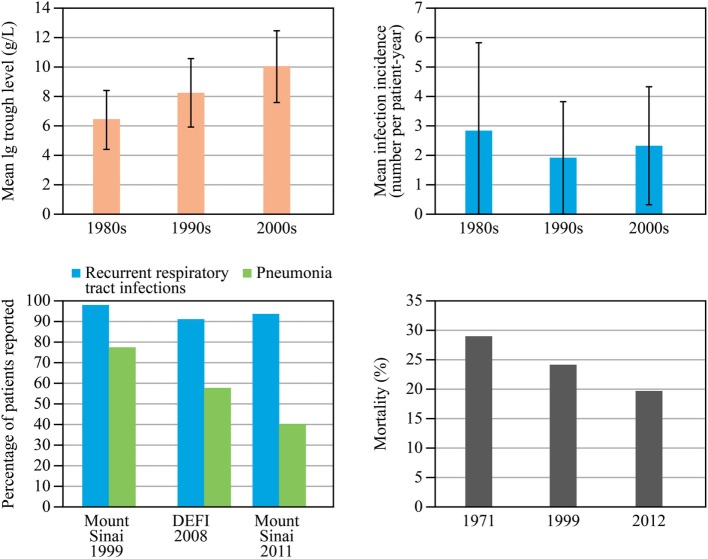
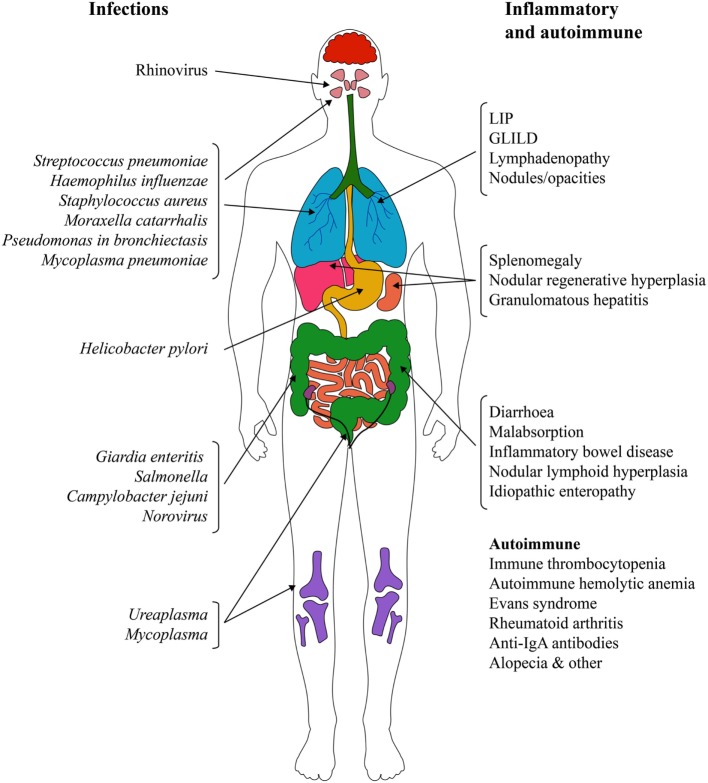
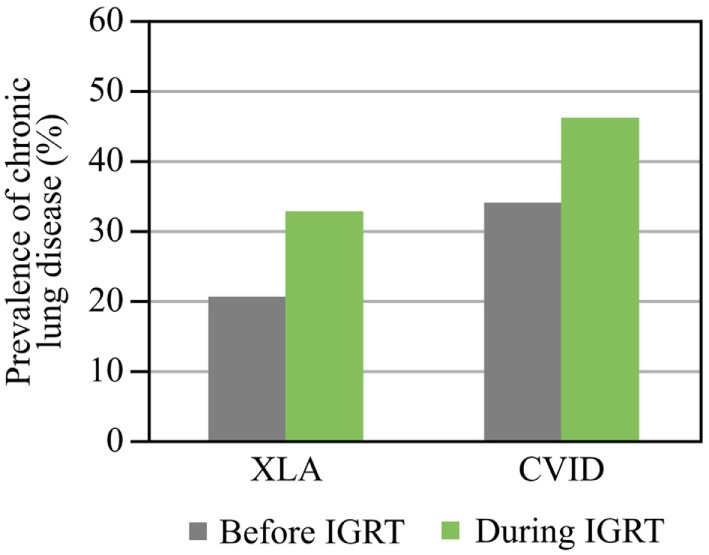
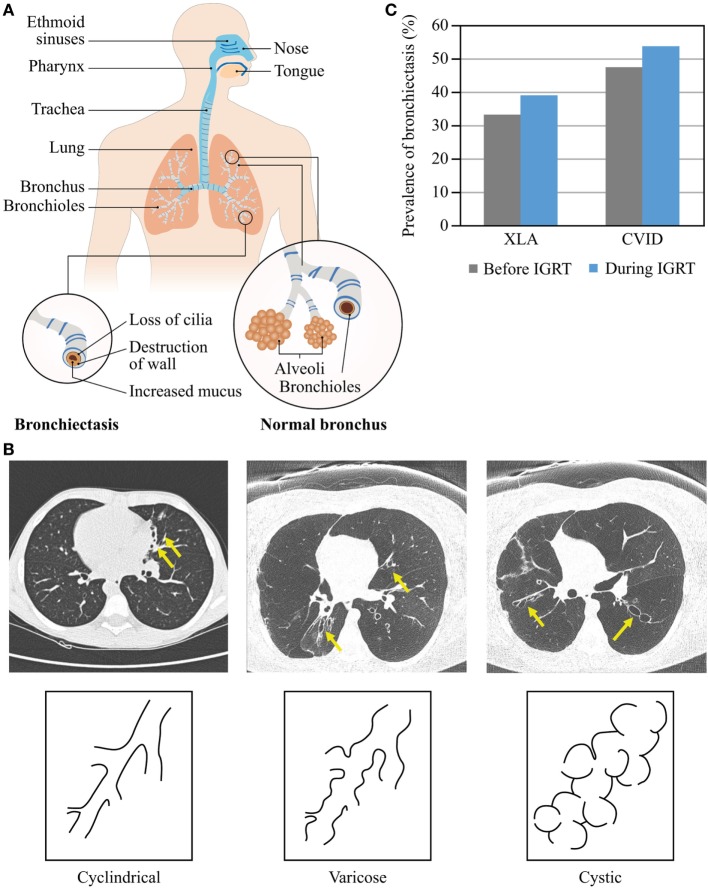
Immunoglobulin replacement therapy (IGRT) has contributed critically to the management of primary antibody deficiencies (PAD) and the decrease in pneumonia rate. However, despite adequate IGRT and improved prognosis, patients with PAD continue to experience recurrent respiratory tract infections, leading to bronchiectasis and continuing decline in lung function with a severe impact on their quality of life. Moreover, non-infectious inflammatory and interstitial lung complications, such as granulomatous-lymphocytic interstitial lung disease, contribute substantially to the overall morbidity of PAD. These conditions develop much more often than appreciated and represent a major therapeutic challenge. Therefore, a regular assessment of the structural and functional condition of the lung and the upper airways with appropriate treatment is required to minimize the deterioration of lung function. This work summarizes the knowledge on lung complications in PAD and discusses the currently available diagnostic tools and treatment options.
Keywords: bronchiectasis; comorbidity; granulomatous-lymphocytic interstitial lung disease; immunoglobulin; lung complications; lung computed tomographic scan; primary immunodeficiency; pulmonary functional tests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources