

The Polycystic Ovary Syndrome and the Metabolic Syndrome: A Possible Chronobiotic-Cytoprotective Adjuvant Therapy
- PMID: 30147722
- PMCID: PMC6083563
- DOI: 10.1155/2018/1349868
The Polycystic Ovary Syndrome and the Metabolic Syndrome: A Possible Chronobiotic-Cytoprotective Adjuvant Therapy
Abstract
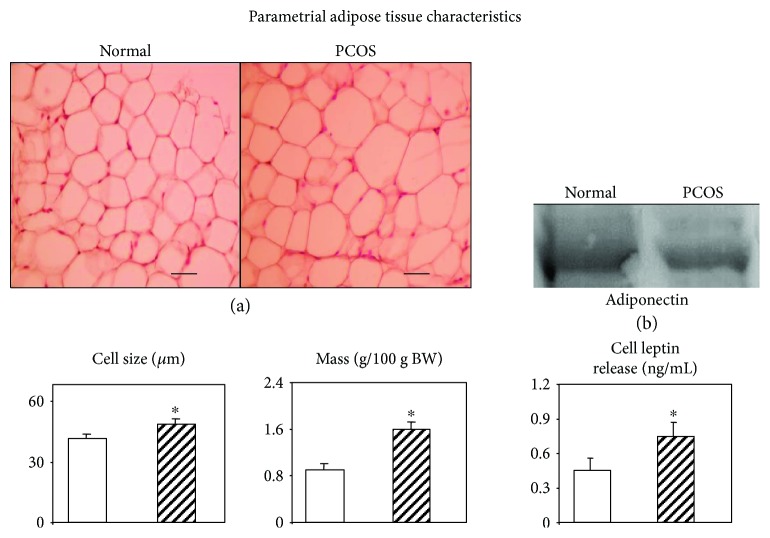
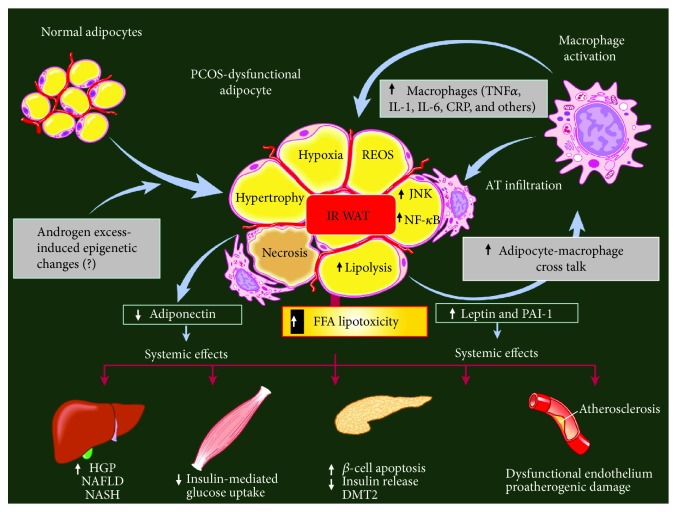
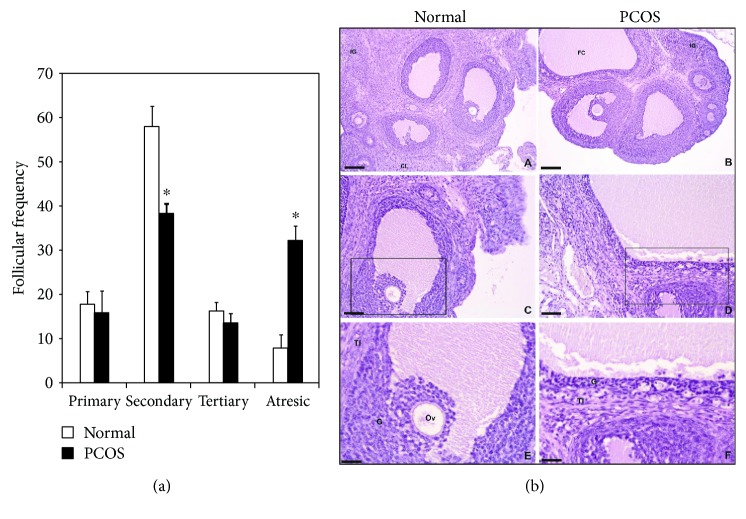
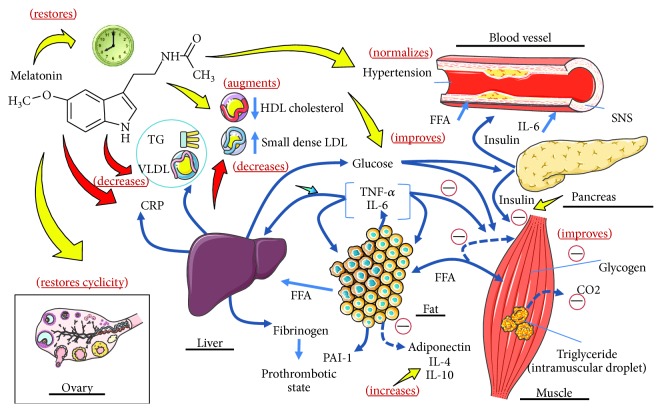
Polycystic ovary syndrome is a highly frequent reproductive-endocrine disorder affecting up to 8-10% of women worldwide at reproductive age. Although its etiology is not fully understood, evidence suggests that insulin resistance, with or without compensatory hyperinsulinemia, and hyperandrogenism are very common features of the polycystic ovary syndrome phenotype. Dysfunctional white adipose tissue has been identified as a major contributing factor for insulin resistance in polycystic ovary syndrome. Environmental (e.g., chronodisruption) and genetic/epigenetic factors may also play relevant roles in syndrome development. Overweight and/or obesity are very common in women with polycystic ovary syndrome, thus suggesting that some polycystic ovary syndrome and metabolic syndrome female phenotypes share common characteristics. Sleep disturbances have been reported to double in women with PCOS and obstructive sleep apnea is a common feature in polycystic ovary syndrome patients. Maturation of the luteinizing hormone-releasing hormone secretion pattern in girls in puberty is closely related to changes in the sleep-wake cycle and could have relevance in the pathogenesis of polycystic ovary syndrome. This review article focuses on two main issues in the polycystic ovary syndrome-metabolic syndrome phenotype development: (a) the impact of androgen excess on white adipose tissue function and (b) the possible efficacy of adjuvant melatonin therapy to improve the chronobiologic profile in polycystic ovary syndrome-metabolic syndrome individuals. Genetic variants in melatonin receptor have been linked to increased risk of developing polycystic ovary syndrome, to impairments in insulin secretion, and to increased fasting glucose levels. Melatonin therapy may protect against several metabolic syndrome comorbidities in polycystic ovary syndrome and could be applied from the initial phases of patients' treatment.
Figures
References
-
- Moran L. J., Pasquali R., Teede H. J., Hoeger K. M., Norman R. J. Treatment of obesity in polycystic ovary syndrome: a position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertility and Sterility. 2009;92(6):1966–1982. doi: 10.1016/j.fertnstert.2008.09.018. - DOI - PubMed
-
- Yildiz B. O., Azziz R., Androgen Excess and PCOS Society Ovarian and adipose tissue dysfunction in polycystic ovary syndrome: report of the 4th special scientific meeting of the Androgen Excess and PCOS Society. Fertility and Sterility. 2010;94(2):690–693. doi: 10.1016/j.fertnstert.2009.03.058. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
