

Risk factors contributing to cardiac events following general and vascular surgery
- PMID: 30147870
- PMCID: PMC6105747
- DOI: 10.1016/j.amsu.2018.08.001
Risk factors contributing to cardiac events following general and vascular surgery
Abstract
Background: Cardiac events (CE) following surgery have been associated with morbidity and mortality. Defining risk factors that contribute to CE is essential to improve surgical outcomes.
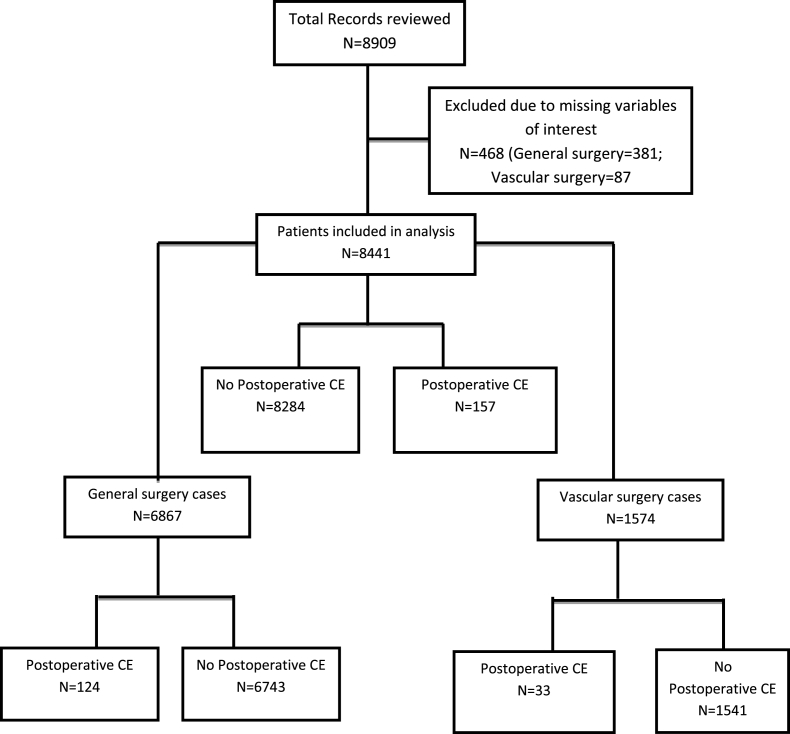
Study design: This was a retrospective study at a large urban teaching hospital for surgery performed from 2013 to 2015. Adult patients (≥18 years) that underwent general and vascular surgery were analyzed. Patients were grouped into those who experienced postoperative CE and those who did not. Univariate and multivariate regression analyses were used to identify predictors of postoperative CE, and association of CE with adverse postoperative outcomes. Separate subgroup analyses were also conducted for general and vascular surgery patients to assess predictors of CE.
Results: Out of 8441 patients, 157 (1.9%) experienced CE after major general and vascular surgery. Underlying predictors for CE included age >65 years(OR 4.9, 95%CI 3.4-6.9,p < 0.01), ASA >3(OR 12.0, 95%CI 8.5-16.9,p < 0.01), emergency surgery(OR 3.7, 95%CI 2.7-5.1,p = 0.01), CHF(OR 11.2, 95%CI 6.4-16.7,p = 0.02), COPD(OR 3.9, 95%CI 2.4-6.4,p = 0.04), acute renal failure or dialysis(OR 8.0, 95%CI 5.2-12.1,p = 0.04), weight loss(OR 3.3, 95%CI 1.7-6.7,p < 0.01), preoperative creatinine >1.2 mg/dL(OR 5.1, 95%CI 3.7-7.1,p = 0.01), hematocrit <34%(OR 4.0, 95%CI 2.8-5.7,p < 0.01), and operative time >240 min(OR 2.0, 95%CI 1.3-3.3,p = 0.02). Following surgery, CE was associated with increased mortality(OR 3.5, 95%CI 1.2-6.5,p < 0.01), pulmonary complications(OR 5.0, 95%CI 3.1-8.9,p < 0.01), renal complications(OR 2.3, 95%CI 1.9-4.5,p < 0.01), neurologic complications(OR 2.5, 95%CI 1.4-5.2,p < 0.01), systemic sepsis(OR 2.2, 95%CI 1.7-4.0,p < 0.01), postoperative RBC transfusion(OR 4.4, 95%CI 2.7-6.5,p < 0.01), unplanned return to operating room(OR 4.0, 95%CI 2.3-6.9,p < 0.01), and prolonged hospitalization (OR 5.5, 95%CI 3.1-8.8,p = 0.03). There was no statistical difference in incidence of CE between general and vascular surgery patients (p = 0.44); however, predictors of CE differed between the two surgical groups.
Conclusion: Postoperative CE are associated with significant morbidity and mortality. Identified predictors of CE should allow for adequate risk stratification and optimization of perioperative surgical management.
Keywords: CE, cardiac events; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; Cardiac events; General surgery; MI, myocardial infarction; Noncardiac surgery; Risk factors; Vascular surgery.
Figures
References
-
- Antman E., Bassand J.P., Klein W. Myocardial infarction redefined—a consensus document of the joint European society of cardiology/American College of cardiology committee for the redefinition of myocardial infarction: the joint European society of cardiology/American College of cardiology committee. J. Am. Coll. Cardiol. 2000;36:959–969. - PubMed
-
- Sprung J., Warner M.E., Contreras M.G. Predictors of survival following cardiac arrest in patients undergoing noncardiac surgery: a study of 518,294 patients at a tertiary referral center. Anesthesiology. 2003;99:259–269. - PubMed
-
- Goldman L., Caldera D.L., Nussbaum S.R. Multifactorial index of cardiac risk in noncardiac surgical procedures. N. Engl. J. Med. 1977;297:845–850. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
