

Chylothorax secondary to venous outflow obstruction treated with transcervical retrograde thoracic duct cannulation with embolization and venous reconstruction
- PMID: 30148237
- PMCID: PMC6105749
- DOI: 10.1016/j.jvscit.2018.03.010
Chylothorax secondary to venous outflow obstruction treated with transcervical retrograde thoracic duct cannulation with embolization and venous reconstruction
Abstract
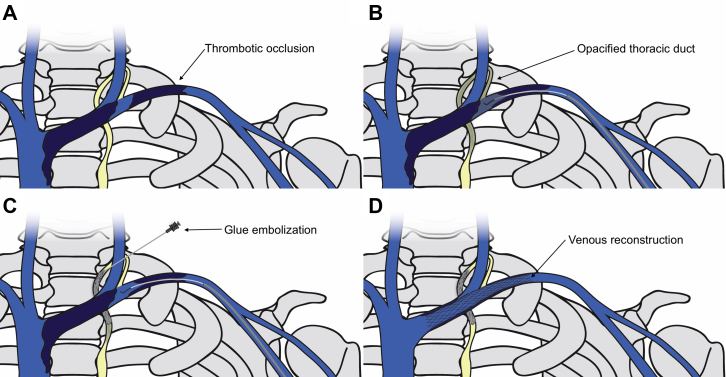
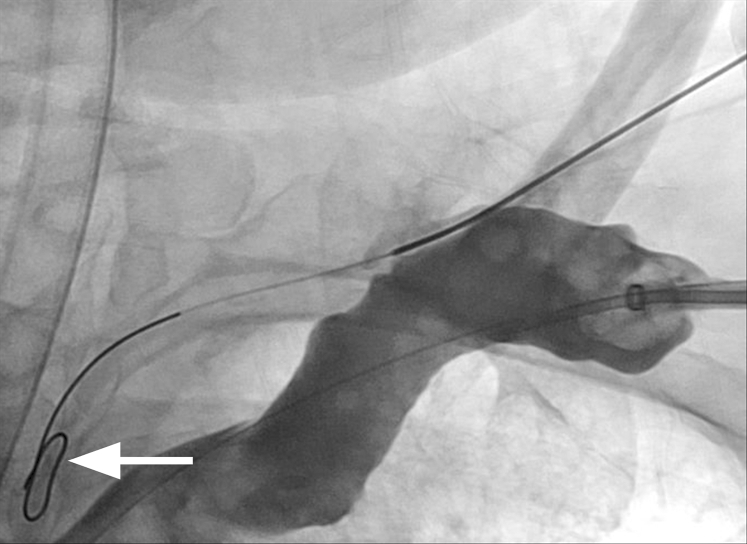
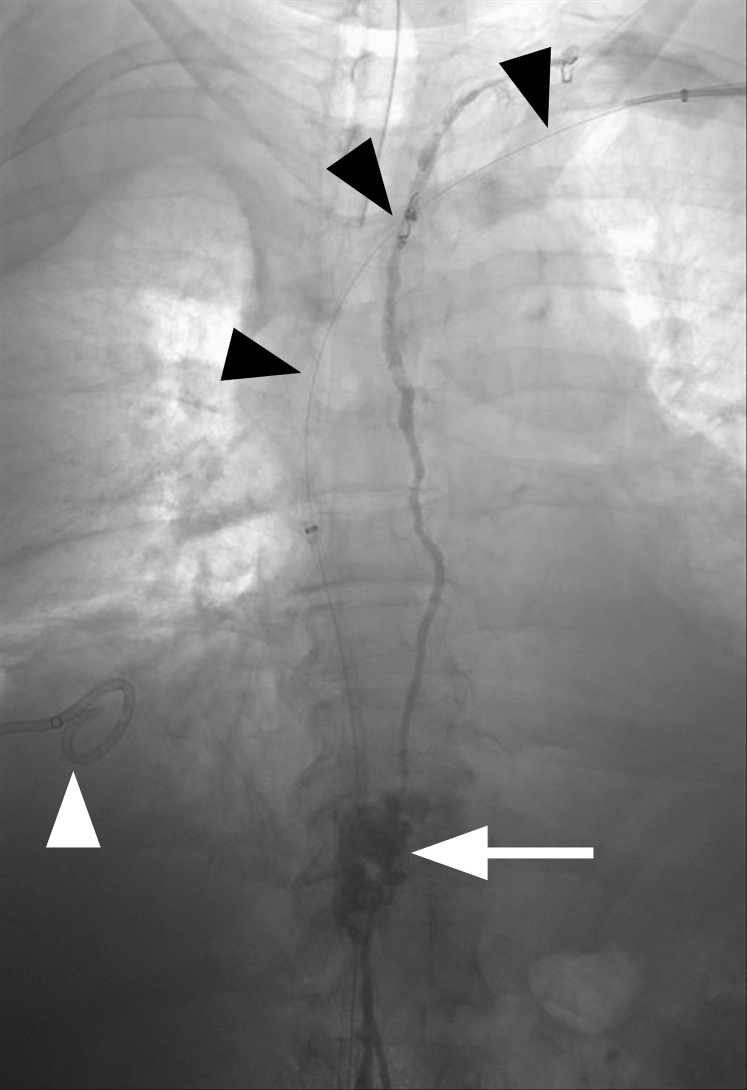
A chylothorax may be due to either direct trauma or occlusion of the thoracic duct. Treatments include antegrade or retrograde glue and coil embolization as well as thoracic duct stent graft placement. This report describes a patient with chylothorax secondary to venous outflow occlusion. Left upper extremity venography demonstrated multifocal left brachiocephalic and axillary vein occlusions with retrograde filling of an engorged and disrupted thoracic duct. Retrograde thoracic duct lymphangiography with embolization and left upper extremity venous reconstruction were performed with complete resolution of chylothorax.
Keywords: Central venous occlusion; Chylothorax; Embolization; Retrograde; Thoracic duct; Venous reconstruction.
Figures




References
-
- Maldonado F., Cartin-Ceba R., Hawkins F.J., Ryu J.H. Medical and surgical management of chylothorax and associated outcomes. Am J Med Sci. 2010;339:314–318. - PubMed
-
- Pamarthi V., Stecker M.S., Schenker M.P., Baum R.A., Killoran T.P., Suzuki Han A. Thoracic duct embolization and disruption for treatment of chylous effusions: experience with 105 patients. J Vasc Interv Radiol. 2014;25:1398–1404. - PubMed
-
- Johnson O.W., Chick J.F., Chauhan N.R., Fairchild A.H., Fan C.M., Stecker M.S. The thoracic duct: clinical importance, anatomic variation, imaging, and embolization. Eur Radiol. 2016;26:2482–2493. - PubMed
-
- Doerr C.H., Allen M.S., Nichols F.C., Ryu J.H. Etiology of chylothorax in 203 patients. Mayo Clin Proc. 2005;80:867–870. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
