

Analysis of MDM2 Amplification: Next-Generation Sequencing of Patients With Diverse Malignancies
- PMID: 30148248
- PMCID: PMC6106866
- DOI: 10.1200/PO.17.00235
Analysis of MDM2 Amplification: Next-Generation Sequencing of Patients With Diverse Malignancies
Abstract
Purpose: MDM2 amplification can promote tumorigenesis directly or indirectly through p53 inhibition. MDM2 has increasing clinical relevance because inhibitors are under evaluation in clinical trials, and MDM2 amplification is a possible genomic correlate of accelerated progression, known as hyperprogression, after anti-PD-1/PD-L1 immunotherapy. We used next-generation sequencing (NGS) to ascertain MDM2 amplification status across a large number of diverse cancers.
Methods: We interrogated the molecular profiles of 102,878 patients with diverse malignancies for MDM2 amplification and co-altered genes using clinical-grade NGS (182 to 465 genes).
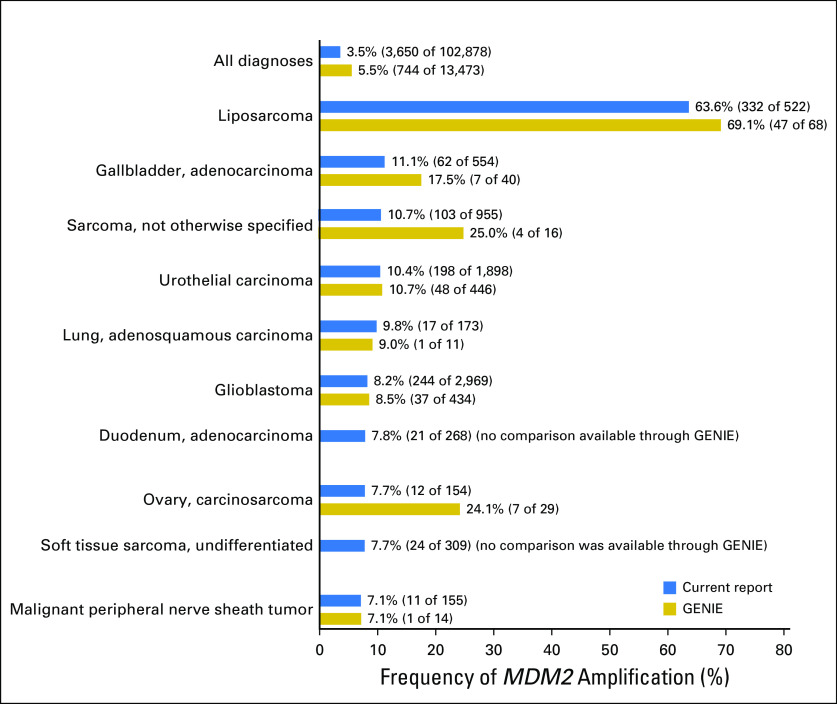
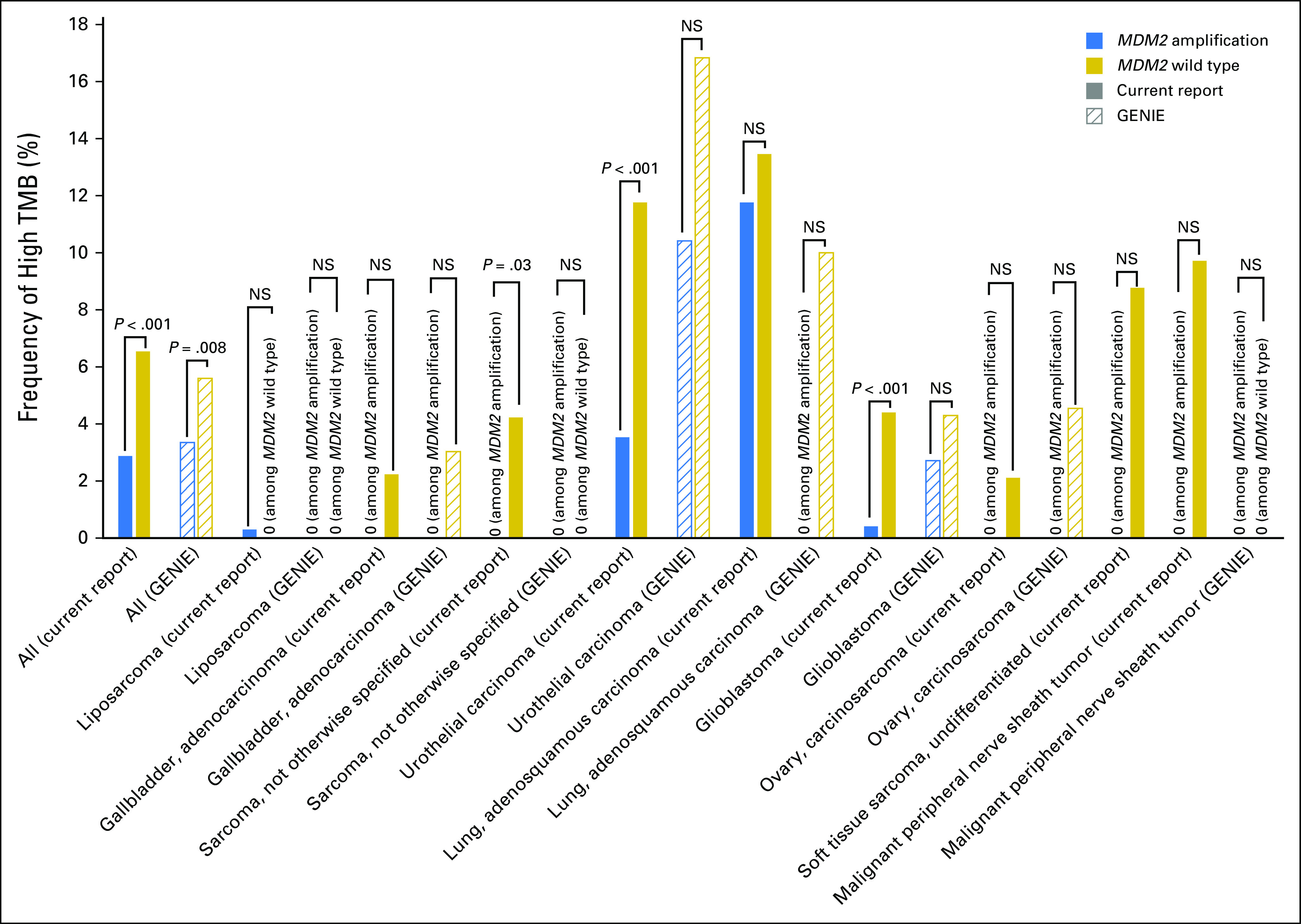
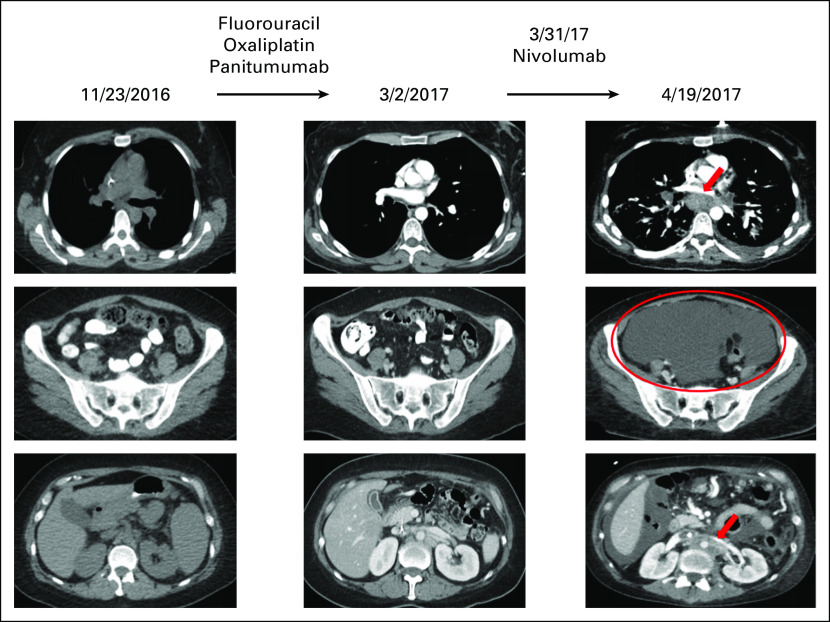
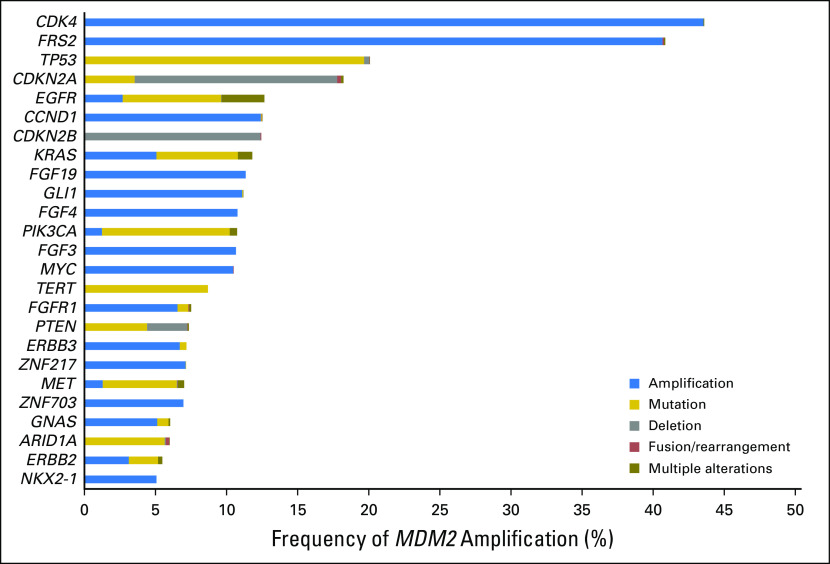
Results: MDM2 amplification occurred in 3.5% of patients (3,650 of 102,878). The majority of tumor types had a small subset of patients with MDM2 amplification. Most of these patients (99.0% [3,613/3,650]) had co-alterations that accompanied MDM2 amplification. Various pathways, including those related to tyrosine kinase (37.9% [1,385 of 3,650]), PI3K signaling (25.4% [926 of 3,650]), TP53 (24.9% [910 of 3,650]), and MAPK signaling (23.6% [863 of 3,650]), were involved. Although infrequent, mismatch repair genes and PD-L1 amplification also were co-altered (2.2% [79 of 3,650]). Most patients (97.6% [3,563 of 3,650]) had one or more co-alterations potentially targetable with either a Food and Drug Administration-approved or investigational agent. MDM2 amplifications were less frequently associated with high tumor mutation burden compared with the MDM2 wild-type population (2.9% v 6.5%; P < .001). An illustrative patient who harbored MDM2 amplification and experienced hyperprogression with an immune checkpoint inhibitor is presented.
Conclusion: MDM2 amplification was found in 3.5% of 102,878 patients, 97.6% of whom harbored genomic co-alterations that were potentially targetable. This study suggests that a small subset of most tumor types have MDM2 amplification as well as pharmacologically tractable co-alterations.
Conflict of interest statement
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO’s conflict of interest policy, please refer to www.asco.org/rwc orascopubs.org/po/author-center.
Figures
References
-
- Chène P. Inhibiting the p53-MDM2 interaction: An important target for cancer therapy. Nat Rev Cancer. 2003;3:102–109. - PubMed
-
- Ito M, Barys L, O’Reilly T, et al. Comprehensive mapping of p53 pathway alterations reveals an apparent role for both SNP309 and MDM2 amplification in sarcomagenesis. Clin Cancer Res. 2011;17:416–426. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
