

Effectiveness of interventions for managing multiple high-burden chronic diseases in older adults: a systematic review and meta-analysis
- PMID: 30150242
- PMCID: PMC6110649
- DOI: 10.1503/cmaj.171391
Effectiveness of interventions for managing multiple high-burden chronic diseases in older adults: a systematic review and meta-analysis
Abstract
Introduction: More than half of older adults (age ≥ 65 yr) have 2 or more high-burden multimorbidity conditions (i.e., highly prevalent chronic diseases, which are associated with increased health care utilization; these include diabetes [DM], dementia, depression, chronic obstructive pulmonary disease [COPD], cardiovascular disease [CVD], arthritis, and heart failure [HF]), yet most existing interventions for managing chronic disease focus on a single disease or do not respond to the specialized needs of older adults. We conducted a systematic review and meta-analysis to identify effective multimorbidity interventions compared with a control or usual care strategy for older adults.
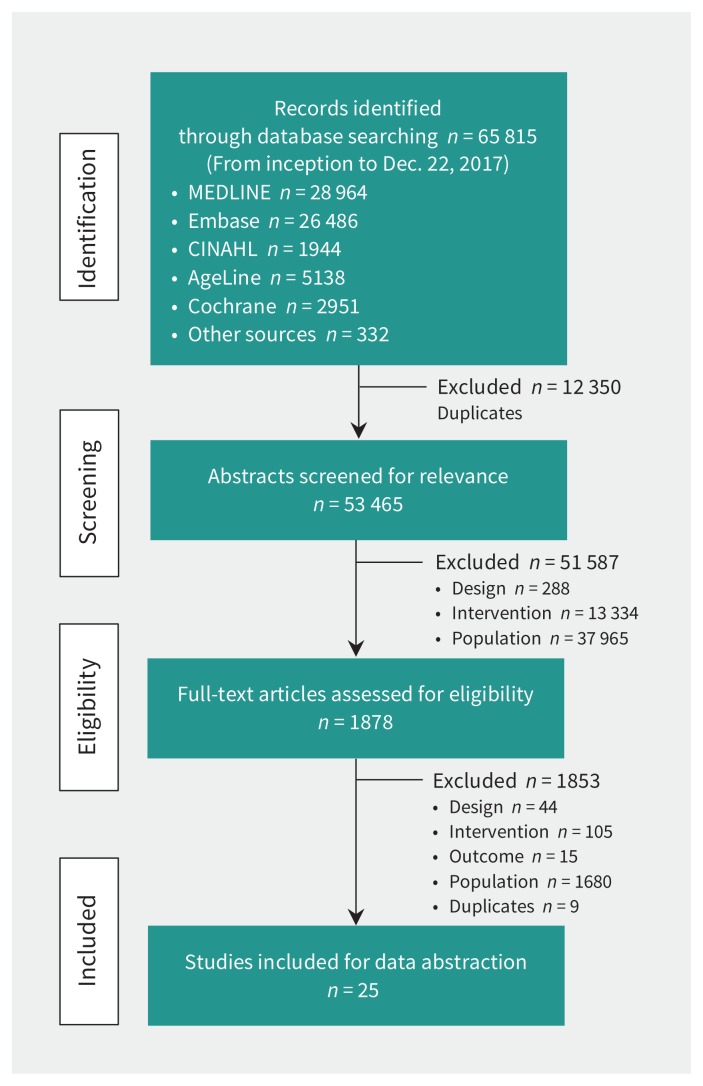
Methods: We searched bibliometric databases for randomized controlled trials (RCTs) evaluating interventions for managing multiple chronic diseases in any language from 1990 to December 2017. The primary outcome was any outcome specific to managing multiple chronic diseases as reported by studies. Reviewer pairs independently screened citations and full-text articles, extracted data and assessed risk of bias. We assessed statistical and methodological heterogeneity and performed a meta-analysis of RCTs with similar interventions and components.
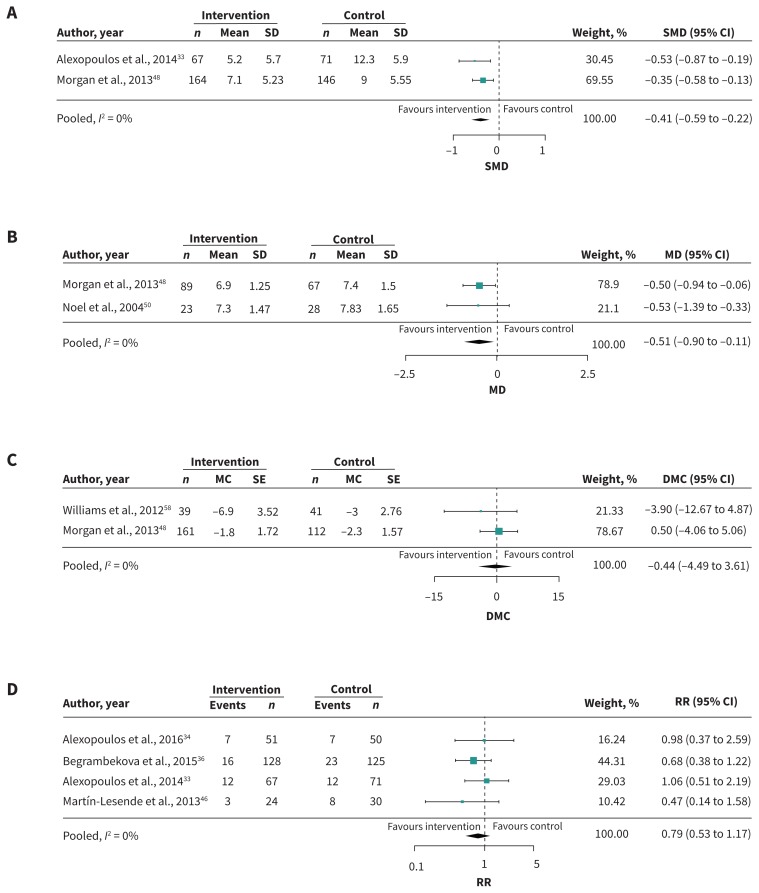
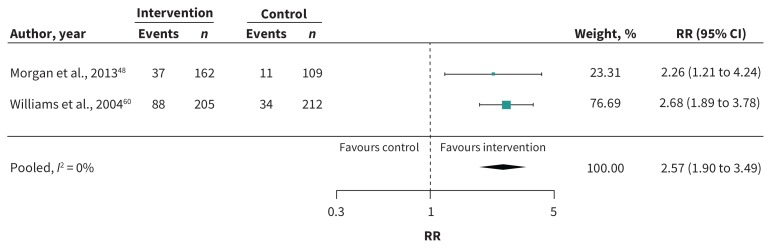
Results: We included 25 studies (including 15 RCTs and 6 cluster RCTs) (12 579 older adults; mean age 67.3 yr). In patients with [depression + COPD] or [CVD + DM], care-coordination strategies significantly improved depressive symptoms (standardized mean difference -0.41; 95% confidence interval [CI] -0.59 to -0.22; I2 = 0%) and reduced glycosylated hemoglobin (HbA1c) levels (mean difference -0.51; 95% CI -0.90 to -0.11; I2 = 0%), but not mortality (relative risk [RR] 0.79; 95% CI 0.53 to 1.17; I2 = 0%). Among secondary outcomes, care-coordination strategies reduced functional impairment in patients with [arthritis + depression] (between-group difference -0.82; 95% CI -1.17 to -0.47) or [DM + depression] (between-group difference 3.21; 95% CI 1.78 to 4.63); improved cognitive functioning in patients with [DM + depression] (between-group difference 2.44; 95% CI 0.79 to 4.09) or [HF + COPD] (p = 0.006); and increased use of mental health services in those with [DM + (CVD or depression)] (RR 2.57; 95% CI 1.90 to 3.49; I2 = 0%).
Interpretation: Subgroup analyses showed that older adults with diabetes and either depression or cardiovascular disease, or with coexistence of chronic obstructive pulmonary disease and heart failure, can benefit from care-coordination strategies with or without education to lower HbA1c, reduce depressive symptoms, improve health-related functional status, and increase the use of mental health services.
Protocol registration: PROSPERO-CRD42014014489.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Noah Ivers reports receiving personal fees and grants from the Canadian Institutes of Health Research and the Government of Ontario during the conduct of the study; he also reports receiving personal fees from Diabetes Canada, outside the submitted work. Noah Ivers held a volunteer position as Chair of the Ontario Vascular Coalition, which envisioned a multicondition approach to management of chronic diseases and risk factors in primary care. Sharon Marr reports a patent issued for the trademark for the Geriatric Certificate program (February 2013). Geoff Wong reports that his salary is partly supported by The Evidence Synthesis Working Group of the National Institute for Health Research School for Primary Care Research (Project Number 390). He is Deputy Chair of the UK National Institute of Health Research Health Technology Assessment Out-of-Hospital Panel. No other competing interests were declared.
Figures
Comment in
-
What we need to learn about multimorbidity.CMAJ. 2018 Aug 27;190(34):E1001. doi: 10.1503/cmaj.181046. CMAJ. 2018. PMID: 30150240 Free PMC article. No abstract available.
-
Assessing methodologic quality of a meta-analysis on managing chronic disease in older adults.CMAJ. 2019 Jun 3;191(22):E617. doi: 10.1503/cmaj.71705. CMAJ. 2019. PMID: 31160500 Free PMC article. No abstract available.
-
The authors respond to "Assessing methodologic quality of a meta-analysis on managing chronic disease in older adults".CMAJ. 2019 Jun 3;191(22):E618. doi: 10.1503/cmaj.72408. CMAJ. 2019. PMID: 31160501 Free PMC article. No abstract available.
References
-
- Canada yearbook. Seniors. Ottawa: Statistics Canada; 2012. Cat no 11-402-X 2012. Available: www.statcan.gc.ca/pub/11-402-x/2012000/chap/seniors-aines/seniorsaines-e... (accessed 2017 May 8).
-
- Major non-communicable diseases and their risk factors. Geneva: World Health Organization; Available: www.who.int/ncds/en/ (accessed 2018 Aug. 9).
-
- Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev 2011;10:430–9. - PubMed
-
- Multimorbidity: technical series on safer primary care. Geneva: World Health Organization; 2016. Available: http://apps.who.int/iris/bitstream/handle/10665/252275/9789241511650-eng... (accessed 2018 Aug. 9).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous