

Seroprevalence, risk factor, and spatial analyses of Zika virus infection after the 2016 epidemic in Managua, Nicaragua
- PMID: 30150394
- PMCID: PMC6140532
- DOI: 10.1073/pnas.1804672115
Seroprevalence, risk factor, and spatial analyses of Zika virus infection after the 2016 epidemic in Managua, Nicaragua
Abstract
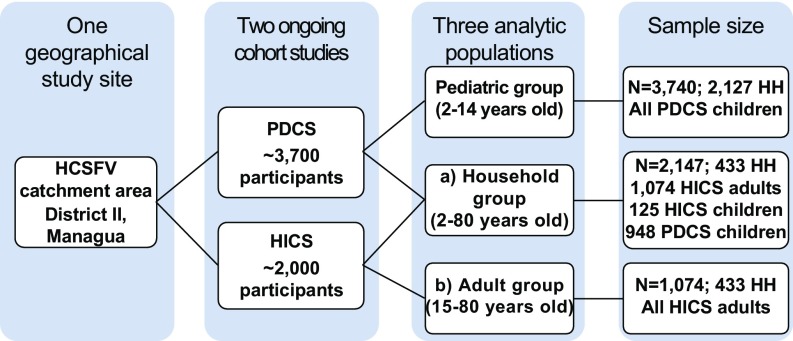
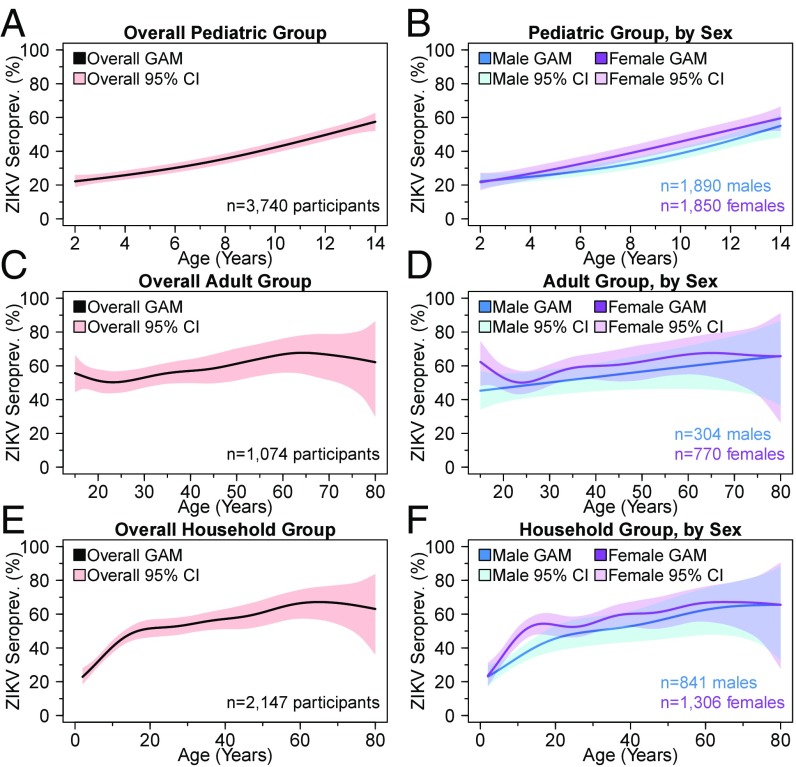
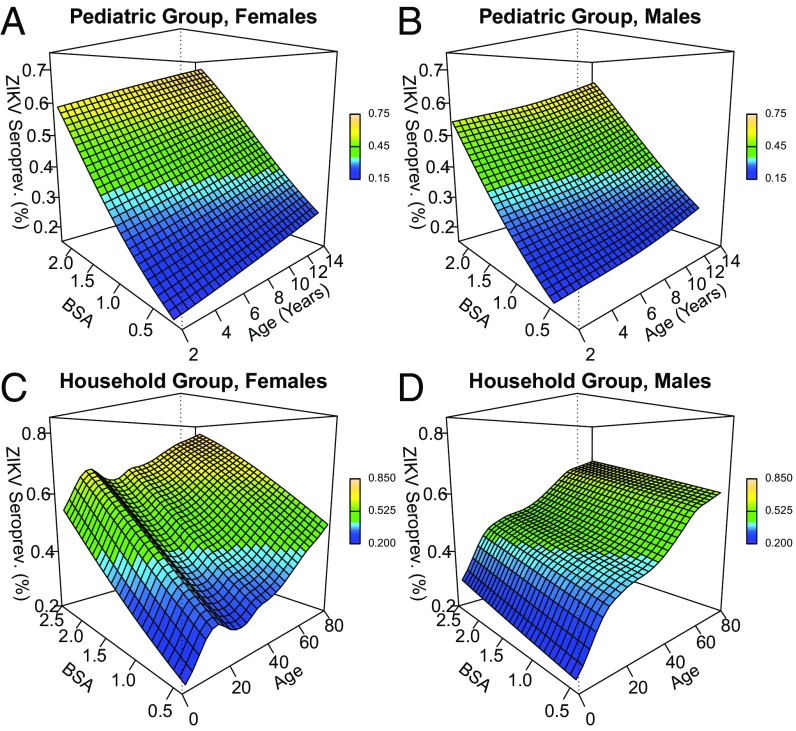
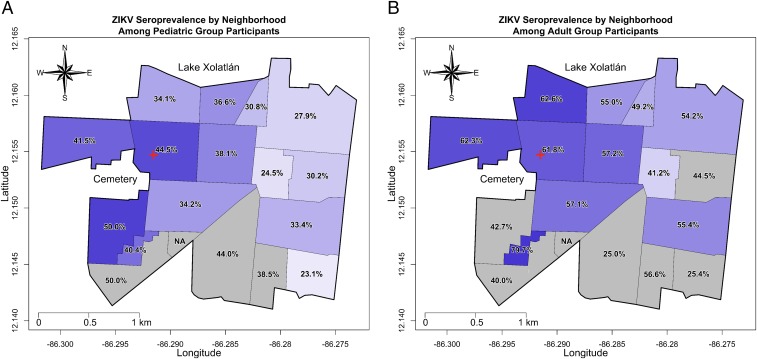
In 2015, a Zika epidemic in Brazil began spreading throughout the Americas. Zika virus (ZIKV) entered Managua, Nicaragua, in January 2016 and caused an epidemic that peaked in July-September 2016. ZIKV seropositivity was estimated among participants of pediatric (n = 3,740) and household (n = 2,147) cohort studies, including an adult-only subset from the household cohort (n = 1,074), in Managua. Seropositivity was based on a highly sensitive and specific assay, the Zika NS1 blockade-of-binding ELISA, which can be used in dengue-endemic populations. Overall seropositivity for the pediatric (ages 2-14), household (ages 2-80), and adult (ages 15-80) cohorts was 36, 46, and 56%, respectively. Trend, risk factor, and contour mapping analyses demonstrated that ZIKV seroprevalence increased nonlinearly with age and that body surface area was statistically associated with increasing seroprevalence in children. ZIKV seropositivity was higher in females than in males across almost all ages, with adjusted prevalence ratios in children and adults of 1.11 (95% CI: 1.02-1.21) and 1.14 (95% CI: 1.01-1.28), respectively. No household-level risk factors were statistically significant in multivariate analyses. A spatial analysis revealed a 10-15% difference in the risk of ZIKV infections across our 3-km-wide study site, suggesting that ZIKV infection risk varies at small spatial scales. To our knowledge, this is the largest ZIKV seroprevalence study reported in the Americas, and the only one in Central America and in children to date. It reveals a high level of immunity against ZIKV in Managua as a result of the 2016 epidemic, making a second large Zika epidemic unlikely in the near future.
Keywords: Zika virus; cohort; risk factor; seroprevalence; spatial analysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- WHO 2016 WHO statement on the first meeting of the International Health Regulations (IHR 2005) Emergency Committee on Zika virus and observed increase in neurological disorders and neonatal malformations: World Health Organization. Available at www.who.int/en/news-room/detail/01-02-2016-who-statement-on-the-first-me.... Accessed January 3, 2018.
-
- Schuler-Faccini L, et al. Brazilian Medical Genetics Society–Zika Embryopathy Task Force Possible association between Zika virus infection and microcephaly: Brazil, 2015. MMWR Morb Mortal Wkly Rep. 2016;65:59–62. - PubMed
-
- Kleber de Oliveira W, et al. Increase in reported prevalence of microcephaly in infants born to women living in areas with confirmed Zika virus transmission during the first trimester of pregnancy: Brazil, 2015. MMWR Morb Mortal Wkly Rep. 2016;65:242–247. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
