

Identification of catheter misplacement in early port CVC dysfunction
- PMID: 30150892
- PMCID: PMC6103231
- DOI: 10.5114/wo.2018.77044
Identification of catheter misplacement in early port CVC dysfunction
Abstract
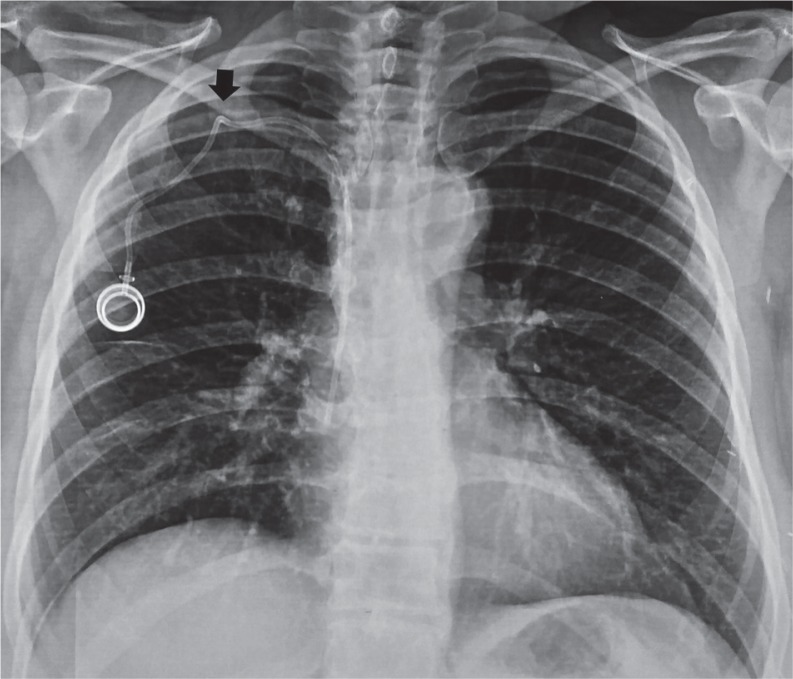
The use of port central venous catheters (CVCs) for chemotherapeutical use has seen exponential growth over the last decades. However, port CVC misplacement may lead to catheter malfunction (such as partial or total catheter blockade), which might be complicated by thrombosis and catheter superinfections, and these in turn may lead to pulmonary embolism and bloodstream infections. The overall occurrence of port CVC misplacement is up to 6%; nonetheless, port CVC misplacement may occur in up to 67% of patients with early CVC dysfunction (occurring within three months of catheter insertion). Thereafter, the prompt evaluation of catheter position among patients with first-trimester CVC dysfunction is extremely important. The aim of the present manuscript is to support medical oncologists, haematologists, and clinicians in timely suspicion and recognition of port CVC misplacement among patients with early CVC dysfunction. Radiological educational iconographic materials that will assist a prompt estimate of port-CVC dislocation are provided.
Keywords: CVCs; central venous catheters; chemotherapy; dysfunction; misplacement; port.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

















References
-
- Sousa B, Furlanetto J, Hutka M, Gouveia P, Wuerstlein R, Mariz JM, Pinto D, Cardoso F, ESMO Guidelines Committee Central venous accesss in Oncology: ESMO Clinical Practice Guidelines. Ann Oncol. 2015;26(Suppl. 5):152–168. - PubMed
-
- Schiffer CA, Mangou PB, Wade JC, et al. Central Venous Catheter care for the patient with cancer: American Society of Clinical Oncology Clinical Practice Guideline. J Clin Oncol. 2013;17:1357–1370. - PubMed
-
- Granic M, Zdravkovic D, Krstajic S, et al. Totally implantable central venous catheters of the port-a-cath type: complications due to its use in the treatment of cancer patients. J BUON. 2014;19:842–846. - PubMed
-
- Mauri D, Roumbkou S, Michalopoulou S, Tsali L, et al. Port central venous catheters associated bloodstream infection during outpatient-based chemotherapy. Med Oncol. 2010;27:1309–1313. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources