

Extrasystoles for fluid responsiveness prediction in critically ill patients
- PMID: 30151211
- PMCID: PMC6103985
- DOI: 10.1186/s40560-018-0324-6
Extrasystoles for fluid responsiveness prediction in critically ill patients
Abstract
Background: Fluid responsiveness prediction with continuously available monitoring is an unsettled matter for the vast majority of critically ill patients, and development of new and reliable methods is desired. We hypothesized that the post-ectopic beat, which is associated with increased preload, could be analyzed in relation to preceding sinus beats and that the change in cardiac performance (e.g., systolic blood pressure) at the post-ectopic beat could predict fluid responsiveness.
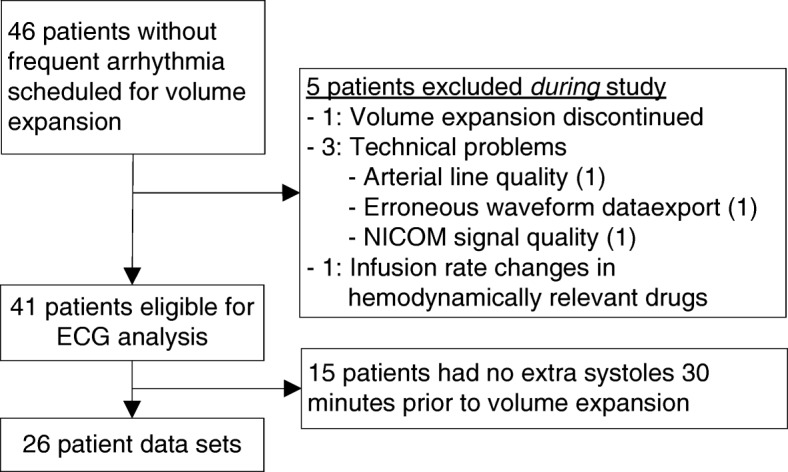
Methods: Critically ill patients were observed when scheduled for a 500-ml volume expansion. The 30-min ECG prior to volume expansion was analyzed for the occurrence of extrasystoles. Classification variables were defined as the change in a variable (e.g., systolic blood pressure or pre-ejection period) from the median of ten preceding sinus beats to extrasystolic post-ectopic beat. A stroke volume increase > 10% following volume expansion defined fluid responsiveness.
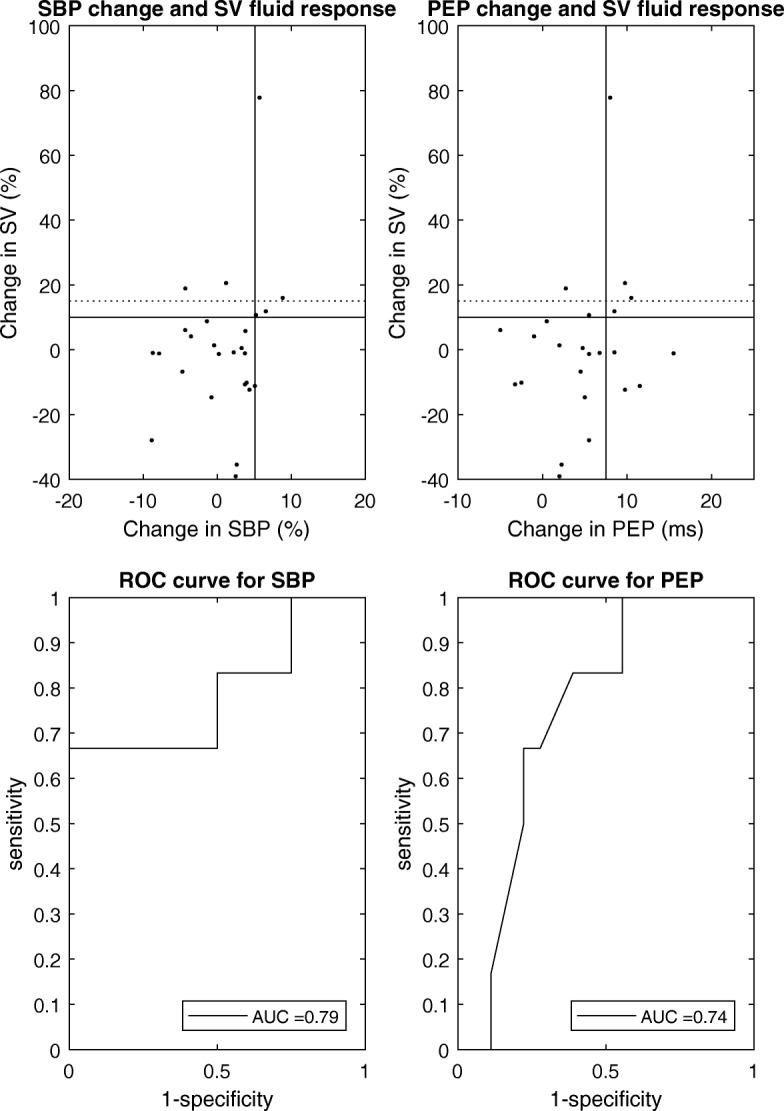
Results: Twenty-six patients were included. The change in systolic blood pressure predicted fluid responsiveness with receiver operating characteristic (ROC) area 0.79 (CI [0.52:1.00]), specificity 100%, sensitivity 67%, positive predictive value 100%, and negative predictive value 91% (threshold: 5%). The change in pre-ejection period predicted fluid responsiveness with ROC area 0.74 (CI [0.53:0.94]), specificity 78%, sensitivity 67%, positive predictive value 50%, and negative predictive value 88% (threshold 7.5 ms).
Conclusions: Based on standard critical care monitoring, analysis of the extrasystolic post-ectopic beat predicts fluid responsiveness in critical care patients with good accuracy. The presented results are considered preliminary proof-of-concept results, and further validation is needed to confirm these preliminary findings.
Keywords: Cardiac output; Ectopic beat; Extrasystole; Fluid responsiveness; Hemodynamic monitoring; Stroke volume.
Conflict of interest statement
The extrasystoles method was previously protected by a patent application owned by Aarhus University (PCT/DK2014/050094; STV as sole inventor). The application did, however, not lead to the granting of a patent at priority expiry date. TWLS is an associate editor of the Journal of Clinical Monitoring and Computing. TWLS received honoraria for consulting from Edwards Lifesciences and Masimo Corp. TWLS is currently the Chair of the Section Cardiovascular Dynamics of the European Society of Intensive Care Medicine as well as the Chair of the Scientific Subcommittee 14 (Monitoring, Ultrasound, and Equipment) of the European Society of Anaesthesiology. Apart from this, all other authors declare that they have no competing interests.This study was exclusively observational and approved as such by the Danish authorities.Not applicableSpringer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Mahjoub Y, Lejeune V, Muller L, Perbet S, Zieleskiewicz L, Bart F, Veber B, Paugam-Burtz C, Jaber S, Ayham A, Zogheib E, Lasocki S, Vieillard-Baron A, Quintard H, Joannes-Boyau O, Plantefeve G, Montravers P, Duperret S, Lakhdari M, Ammenouche N, Lorne E, Slama M, Dupont H. Evaluation of pulse pressure variation validity criteria in critically ill patients: a prospective observational multicentre point-prevalence study. Br J Anaesth. 2014;112(4):681–685. doi: 10.1093/bja/aet442. - DOI - PubMed
-
- Cavallaro F, Sandroni C, Marano C, La Torre G, Mannocci A, De Waure C, Bello G, Maviglia R, Antonelli M. Diagnostic accuracy of passive leg raising for prediction of fluid responsiveness in adults: systematic review and meta-analysis of clinical studies. Intensive Care Med. 2010;36(9):1475–1483. doi: 10.1007/s00134-010-1929-y. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
