

Prevalence and Transmission Dynamics of HIV-1 Transmitted Drug Resistance in a Southeastern Cohort
- PMID: 30151407
- PMCID: PMC6101542
- DOI: 10.1093/ofid/ofy178
Prevalence and Transmission Dynamics of HIV-1 Transmitted Drug Resistance in a Southeastern Cohort
Abstract
Background: Transmitted drug resistance (TDR) compromises clinical management and outcomes. Transmitted drug resistance surveillance and identification of growing transmission clusters are needed in the Southeast, the epicenter of the US HIV epidemic. Our study investigated prevalence and transmission dynamics in North Carolina.
Methods: We analyzed surveillance drug resistance mutations (SDRMs) using partial pol sequences from patients presenting to 2 large HIV outpatient clinics from 1997 to 2014. Transmitted drug resistance prevalence was defined as ≥1 SDRMs among antiretroviral therapy (ART)-naïve patients. Binomial regression was used to characterize prevalence by calendar year, drug class, and demographic and clinical factors. We assessed the transmission networks of patients with TDR with maximum likelihood trees and Bayesian methods including background pol sequences (n = 15 246).
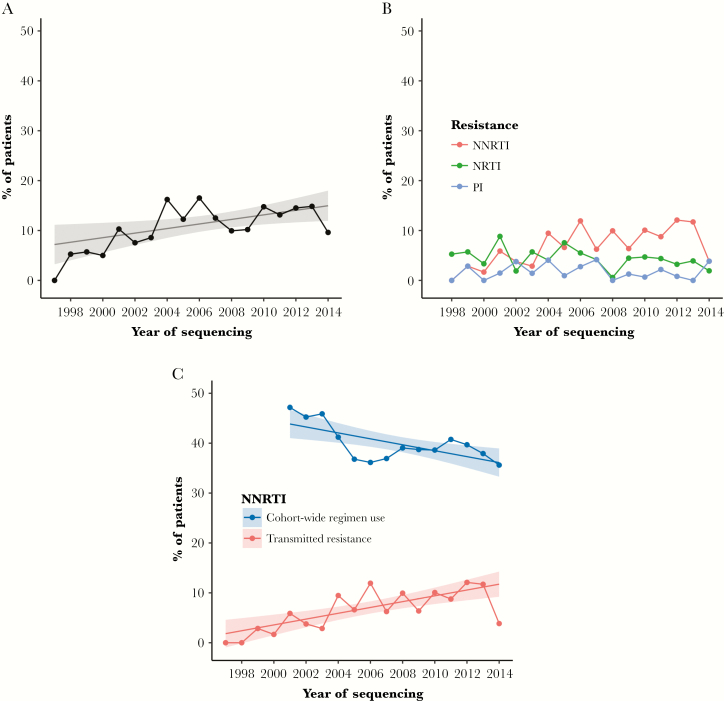
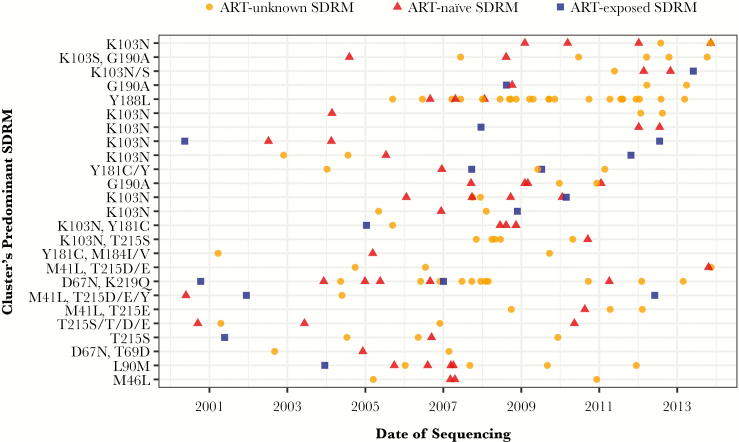
Results: Among 1658 patients with pretherapy resistance testing, ≥1 SDRMs was identified in 199 patients, with an aggregate TDR prevalence of 12% (95% confidence interval, 10% to 14%) increasing over time (P = .02). Resistance to non-nucleoside reverse transcriptase inhibitors (NNRTIs; 8%) was common, followed by nucleoside reverse transcriptase inhibitors (4%) and protease inhibitors (2%). Factors associated with TDR were being a man reporting sex with men, white race, young age, higher CD4 cell count, and being a member of a transmission cluster. Transmitted drug resistance was identified in 106 clusters ranging from 2 to 26 members. Cluster resistance was primarily NNRTI and dominated by ART-naïve patients or those with unknown ART initiation.
Conclusions: Moderate TDR prevalence persists in North Carolina, predominantly driven by NNRTI resistance. Most TDR cases were identified in transmission clusters, signifying multiple local transmission networks and TDR circulation among ART-naïve persons. Transmitted drug resistance surveillance can detect transmission networks and identify patients for enhanced services to promote early treatment.
Keywords: HIV-1; Southeastern United States; antiretroviral therapy; drug resistance; molecular epidemiology.
Figures
References
-
- Wittkop L, Günthard HF, de Wolf F, et al. ; EuroCoord-CHAIN Study Group Effect of transmitted drug resistance on virological and immunological response to initial combination antiretroviral therapy for HIV (EuroCoord-CHAIN joint project): a European multicohort study. Lancet Infect Dis 2011; 11:363–71. - PubMed
-
- Yang WL, Kouyos R, Scherrer AU, et al. ; Swiss HIV Cohort Study Assessing the paradox between transmitted and acquired HIV type 1 drug resistance mutations in the Swiss HIV Cohort Study from 1998 to 2012. J Infect Dis 2015; 212:28–38. - PubMed
-
- Bertagnolio S, Perno CF, Vella S, Pillay D. The impact of HIV drug resistance on the selection of first- and second-line ART in resource-limited settings. J Infect Dis 2013; 207(Suppl 2):S45–8. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
