

Cerebellovascular Disease: Magnetic Resonance Imaging
- PMID: 30151488
- PMCID: PMC6100669
- DOI: 10.5334/jbr-btr.1230
Cerebellovascular Disease: Magnetic Resonance Imaging
Abstract
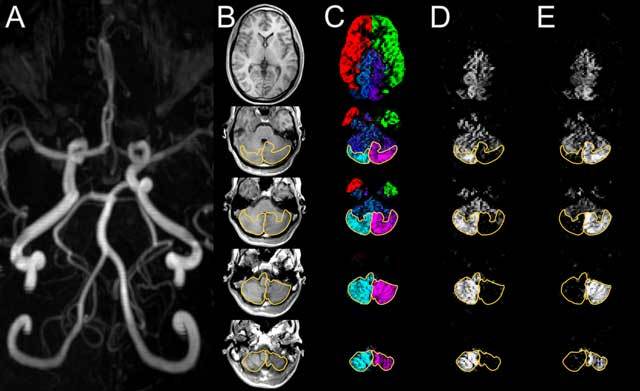
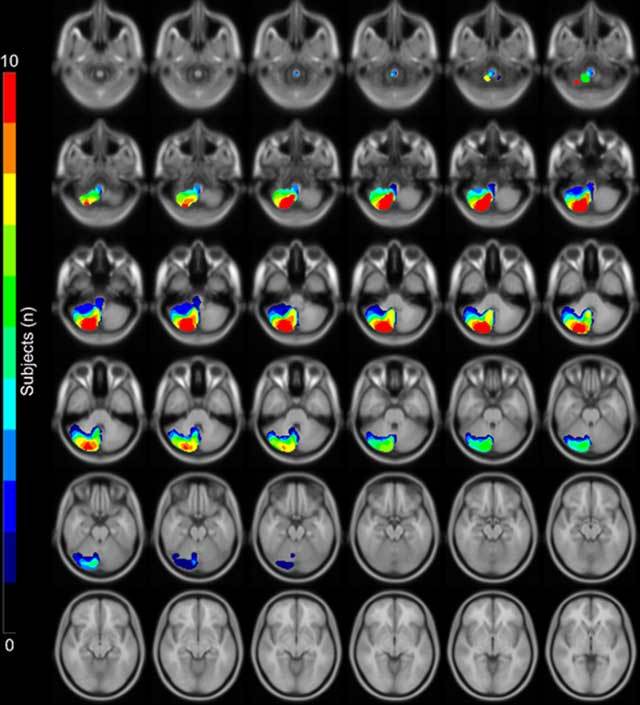
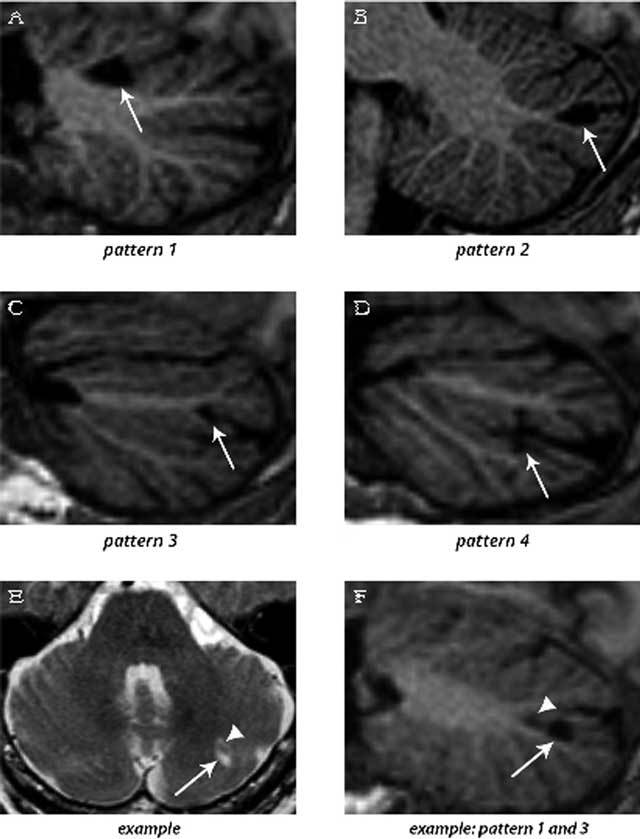
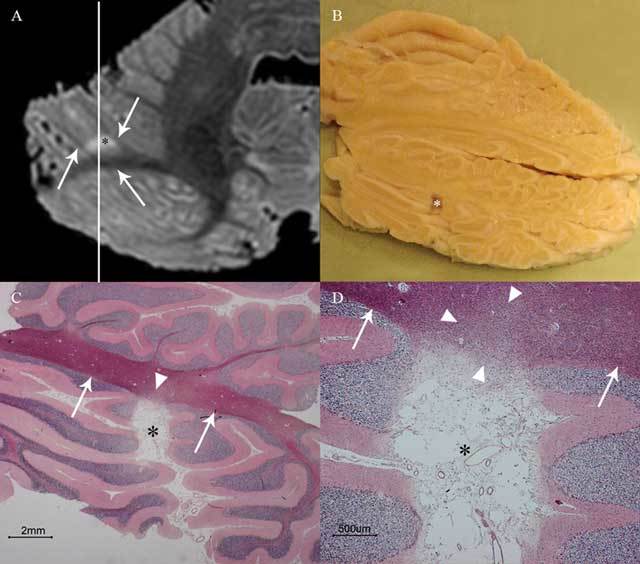
The goal of this thesis was to elucidate the details of cerebellovascular diseases with advanced magnetic resonance (MR) imaging (MRI) and to translate the findings to routine clinical MRI. The first aim was to image cerebellar arterial perfusion territories, which was achieved by applying super-selective arterial spin labelling (ASL) MRI with labelling of both vertebral arteries in addition to the carotid arteries. The second aim was to unravel the imaging patterns of cerebellar infarctions with 7T post-mortem MRI in addition to volume (3D) clinical MRI. This research led to the description of "cerebellar cortical infarct cavities", an incidental imaging finding that proved to be the most frequent manifestation of cerebellar ischemia as well as a marker of atherosclerotic and thromboembolic cerebrovascular disease. Finally, we found that almost all patients with such cavities lack a clinical history of vertebrobasilar transient ischemic attack (TIA) or stroke, disclosing the still very high incidence of clinically occult ischemia in the posterior fossa.
Keywords: 7-Tesla MRI; Arterial Spin Labeling; MRI; PICA; cerebellum; infarct.
Figures

References
-
- Bokkers RP, De Cocker LJ, van Osch MJP, Hartkamp NS, Hendrikse J. Selective arterial spin labeling: Techniques and neurovascular applications. Top Magn Reson Imaging. 2016;25:73–80. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
