

Lateral Subcutaneous Locking Compression Plate and Small Incision Reduction for Distal-third Diaphyseal Humerus Fractures
- PMID: 30152611
- PMCID: PMC6175191
- DOI: 10.1111/os.12398
Lateral Subcutaneous Locking Compression Plate and Small Incision Reduction for Distal-third Diaphyseal Humerus Fractures
Abstract
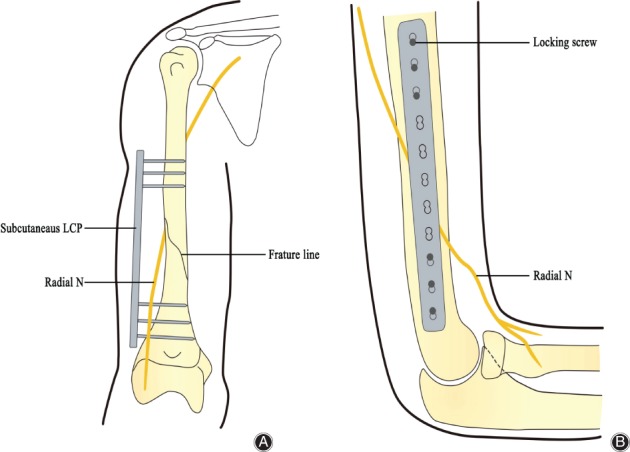
Objective: Iatrogenic radial nerve injury is a great challenge for orthopaedic surgeons who deal with distal-third diaphyseal humerus fractures. Conventional open reduction and internal fixation (ORIF) remains the gold standard, but complications such as nonunion and iatrogenic radial nerve injury still occur. We fixed the fractures with a lateral locking compression plate (LCP) subcutaneously after small incision reduction to protect the radial nerve. This study reports the clinical and radiographic outcomes of our modified method.
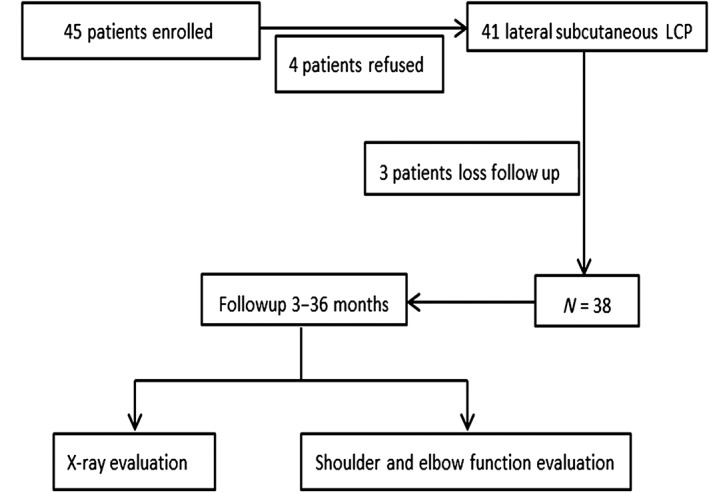
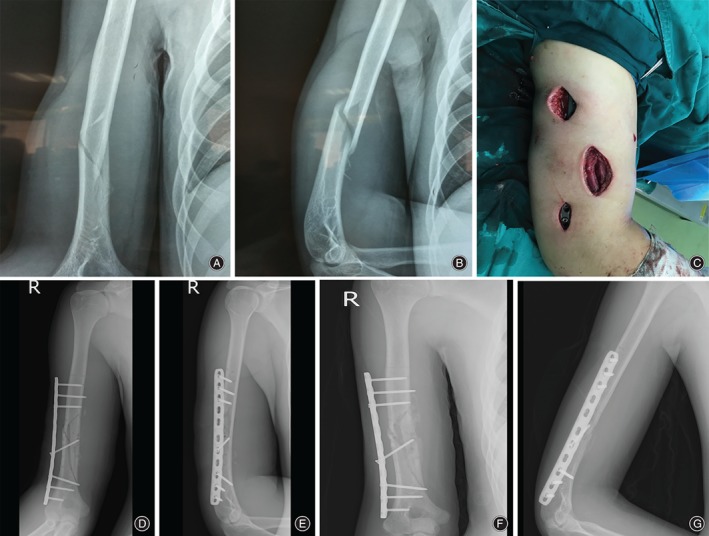
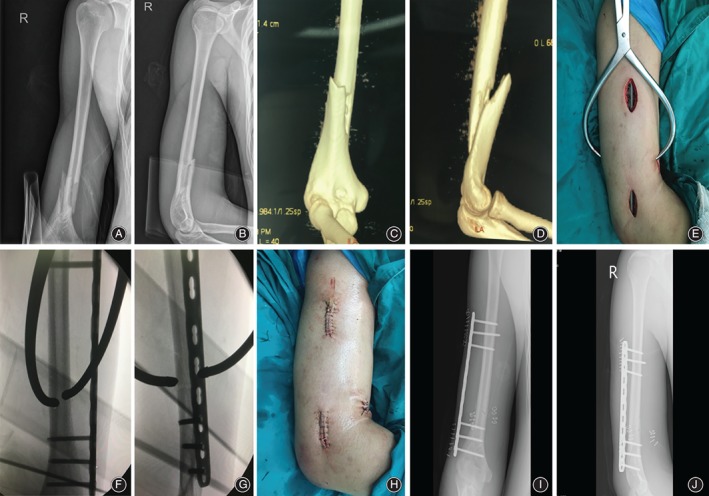
Methods: Thirty-eight patients with distal-third diaphyseal humerus fractures were treated with lateral subcutaneous LCP and small incision reduction at our department between September 2013 and August 2016. There were 33 males and 5 females, with an average age of 30.3 years (range, 17 to 49 years). All the cases were types A or B (AO/OTA classification, type A, 24 cases; type B, 14 cases). Among them, 6 cases were combined with preoperative radial nerve palsy. All patients were diagnosed with closed humeral fractures after X-ray examination, and had typical upper limb pain, swelling, and movement disorders. The operations were performed by a single surgeons' team. Union time, range of motion (ROM), University of California, Los Angeles (UCLA) shoulder rating scale, and Mayo Elbow Performance Index (MEPI) scores were assessed to evaluate the postoperative results.
Results: All patients were followed up for an average of 11.4 months (range, 3 to 36 months). The average operation time was 75.5 min (range, 60 to 150 min) and average intraoperative radiation exposure was 10.5 s (range, 8 to 18 s). Bony union was achieved in all cases after an average of 16.2 weeks (range, 12 to 25 weeks). No complications such as infection or screw and plate fracture occurred, and no iatrogenic radial nerve injury was observed. According to the UCLA shoulder rating scale, the average score was 33.7 (range, 31 to 35), with 33 excellent (86.8%) and 5 good cases (13.2%). They were all excellent according to their MEPI scores (ranging, 94 to 100, with an average of 97.4). The average operation time for secondary removal of the plate was 15.2 min (range, 10 to 20 min), and no complications such as infection or secondary radial nerve injury occurred.
Conclusions: Lateral subcutaneous LCP and small incision reduction may reduce the risk of iatrogenic radial nerve injury significantly in the treatment of distal-third diaphyseal humerus fractures. It also leads to solid fixation, good postoperative function, and convenient removal of the plate without injuring the radial nerve.
Keywords: Humeral fracture; Locking compression plate; Small incision reduction; Subcutaneous.
© 2018 The Authors Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures
Similar articles
-
Antero-lateral minimally invasive plate osteosynthesis (MIPO) with the radial nerve exploration for extra-articular distal-third diaphyseal fractures of the humerus.Int Orthop. 2017 Sep;41(9):1757-1762. doi: 10.1007/s00264-017-3514-2. Epub 2017 Jun 2. Int Orthop. 2017. PMID: 28577034
-
Minimally Invasive Plate Osteosynthesis Using a Screw Compression Method for Treatment of Humeral Shaft Fractures.Clin Orthop Surg. 2017 Dec;9(4):506-513. doi: 10.4055/cios.2017.9.4.506. Epub 2017 Nov 10. Clin Orthop Surg. 2017. PMID: 29201304 Free PMC article.
-
Dual plate fixation on distal third diaphyseal fracture of the humerus.Int Orthop. 2017 Aug;41(8):1655-1661. doi: 10.1007/s00264-016-3355-4. Epub 2016 Dec 1. Int Orthop. 2017. PMID: 27909754
-
[Fractures of the shaft of the humerus: systematic plate fixation. Anatomic and functional results in 156 cases and a review of the literature].Rev Chir Orthop Reparatrice Appar Mot. 2000 Jun;86(4):346-59. Rev Chir Orthop Reparatrice Appar Mot. 2000. PMID: 10880934 Review. French.
-
The Outcomes of Intra-Articular Distal Humerus Open Reduction and Internal Fixation Using Parallel Precontoured Plates in the Elderly.J Hand Surg Am. 2023 Aug;48(8):830.e1-830.e8. doi: 10.1016/j.jhsa.2022.01.030. Epub 2022 Apr 7. J Hand Surg Am. 2023. PMID: 35400538 Review.
Cited by
-
Surgical approach for fracture of distal humerus: Posterior vs lateral.Orthop Rev (Pavia). 2020 Jun 25;12(Suppl 1):8664. doi: 10.4081/or.2020.8664. eCollection 2020 Jun 29. Orthop Rev (Pavia). 2020. PMID: 32913599 Free PMC article.
-
Clinical efficacy of internal fixation with locking compression plates in the treatment of patients with extremity fractures and the effect on the recovery of limb function.Medicine (Baltimore). 2023 Dec 1;102(48):e35884. doi: 10.1097/MD.0000000000035884. Medicine (Baltimore). 2023. PMID: 38050232 Free PMC article.
-
In cases of humeral diaphyseal fractures, is lateral approach surgery without radial nerve exploration as effective and safe as conventional surgery?Ulus Travma Acil Cerrahi Derg. 2024 Jun;30(6):451-457. doi: 10.14744/tjtes.2024.49500. Ulus Travma Acil Cerrahi Derg. 2024. PMID: 38863290 Free PMC article.
References
-
- Jawa A, McCarty P, Doornberg J, Harris M, Ring D. Extra‐articular distal‐third diaphyseal fractures of the humerus. A comparison of functional bracing and plate fixation. J Bone Joint Surg Am, 2006, 88: 2343–2347. - PubMed
-
- Davies G, Yeo G, Meta M, Miller D, Hohmann E, Tetsworth K. Case‐match controlled comparison of minimally invasive plate Osteosynthesis and intramedullary nailing for the stabilization of humeral shaft fractures. J Orthop Trauma, 2016, 30: 612–617. - PubMed
-
- Hohmann E, Glatt V, Tetsworth K. Minimally invasive plating versus either open reduction and plate fixation or intramedullary nailing of humeral shaft fractures: a systematic review and meta‐analysis of randomized controlled trials. J Shoulder Elbow Surg, 2016, 25: 1634–1642. - PubMed
-
- Scaglione M, Fabbri L, Dell, Omo D, Goffi A, Guido G. The role of external fixation in the treatment of humeral shaft fractures: a retrospective case study review on 85 humeral fractures. Injury, 2015, 46: 265–269. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
