

Relationship between very low low-density lipoprotein cholesterol concentrations not due to statin therapy and risk of type 2 diabetes: A US-based cross-sectional observational study using electronic health records
- PMID: 30153257
- PMCID: PMC6112635
- DOI: 10.1371/journal.pmed.1002642
Relationship between very low low-density lipoprotein cholesterol concentrations not due to statin therapy and risk of type 2 diabetes: A US-based cross-sectional observational study using electronic health records
Abstract
Background: Observations from statin clinical trials and from Mendelian randomization studies suggest that low low-density lipoprotein cholesterol (LDL-C) concentrations may be associated with increased risk of type 2 diabetes mellitus (T2DM). Despite the findings from statin clinical trials and genetic studies, there is little direct evidence implicating low LDL-C concentrations in increased risk of T2DM.
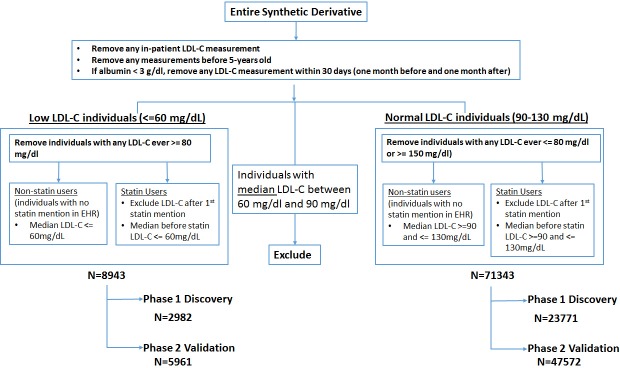
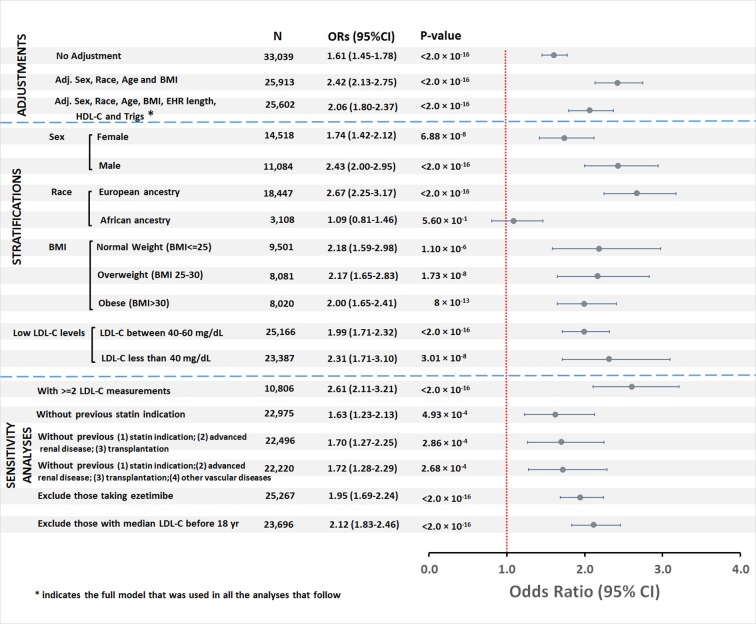
Methods and findings: We used de-identified electronic health records (EHRs) at Vanderbilt University Medical Center to compare the risk of T2DM in a cross-sectional study among individuals with very low (≤60 mg/dl, N = 8,943) and normal (90-130 mg/dl, N = 71,343) LDL-C levels calculated using the Friedewald formula. LDL-C levels associated with statin use, hospitalization, or a serum albumin level < 3 g/dl were excluded. We used a 2-phase approach: in 1/3 of the sample (discovery) we used T2DM phenome-wide association study codes (phecodes) to identify cases and controls, and in the remaining 2/3 (validation) we identified T2DM cases and controls using a validated algorithm. The analysis plan for the validation phase was constructed at the time of the design of that component of the study. The prevalence of T2DM in the very low and normal LDL-C groups was compared using logistic regression with adjustment for age, race, sex, body mass index (BMI), high-density lipoprotein cholesterol, triglycerides, and duration of care. Secondary analyses included prespecified stratification by sex, race, BMI, and LDL-C level. In the discovery cohort, phecodes related to T2DM were significantly more frequent in the very low LDL-C group. In the validation cohort (N = 33,039 after applying the T2DM algorithm to identify cases and controls), the risk of T2DM was increased in the very low compared to normal LDL-C group (odds ratio [OR] 2.06, 95% CI 1.80-2.37; P < 2 × 10-16). The findings remained significant in sensitivity analyses. The association between low LDL-C levels and T2DM was significant in males (OR 2.43, 95% CI 2.00-2.95; P < 2 × 10-16) and females (OR 1.74, 95% CI 1.42-2.12; P = 6.88 × 10-8); in normal weight (OR 2.18, 95% CI 1.59-2.98; P = 1.1× 10-6), overweight (OR 2.17, 95% CI 1.65-2.83; P = 1.73× 10-8), and obese (OR 2.00, 95% CI 1.65-2.41; P = 8 × 10-13) categories; and in individuals with LDL-C < 40 mg/dl (OR 2.31, 95% CI 1.71-3.10; P = 3.01× 10-8) and LDL-C 40-60 mg/dl (OR 1.99, 95% CI 1.71-2.32; P < 2.0× 10-16). The association was significant in individuals of European ancestry (OR 2.67, 95% CI 2.25-3.17; P < 2 × 10-16) but not in those of African ancestry (OR 1.09, 95% CI 0.81-1.46; P = 0.56). A limitation was that we only compared groups with very low and normal LDL-C levels; also, since this was not an inception cohort, we cannot exclude the possibility of reverse causation.
Conclusions: Very low LDL-C concentrations occurring in the absence of statin treatment were significantly associated with T2DM risk in a large EHR population; this increased risk was present in both sexes and all BMI categories, and in individuals of European ancestry but not of African ancestry. Longitudinal cohort studies to assess the relationship between very low LDL-C levels not associated with lipid-lowering therapy and risk of developing T2DM will be important.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Association of Lipoproteins, Insulin Resistance, and Rosuvastatin With Incident Type 2 Diabetes Mellitus : Secondary Analysis of a Randomized Clinical Trial.JAMA Cardiol. 2016 May 1;1(2):136-45. doi: 10.1001/jamacardio.2016.0096. JAMA Cardiol. 2016. PMID: 27347563 Free PMC article. Clinical Trial.
-
Status of lipid control in Bangladeshi subjects with type 2 diabetes mellitus on lipid-lowering drugs: a multicenter, facility-based, cross-sectional study.BMC Endocr Disord. 2023 Dec 5;23(1):268. doi: 10.1186/s12902-023-01522-z. BMC Endocr Disord. 2023. PMID: 38053073 Free PMC article.
-
Lipid traits and type 2 diabetes risk in African ancestry individuals: A Mendelian Randomization study.EBioMedicine. 2022 Apr;78:103953. doi: 10.1016/j.ebiom.2022.103953. Epub 2022 Mar 21. EBioMedicine. 2022. PMID: 35325778 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Lipid Screening in Childhood for Detection of Multifactorial Dyslipidemia: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Aug. Report No.: 14-05204-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2016 Aug. Report No.: 14-05204-EF-1. PMID: 27559550 Free Books & Documents. Review.
Cited by
-
Low levels of low-density lipoprotein cholesterol, intracerebral haemorrhage, and other safety issues: is there still a matter of debate?Eur Heart J Open. 2022 Jun 7;2(4):oeac038. doi: 10.1093/ehjopen/oeac038. eCollection 2022 Jul. Eur Heart J Open. 2022. PMID: 36117951 Free PMC article.
-
LDL Cholesterol and Dysglycemia: an Intriguing Physiological Relationship.Diabetes. 2020 Oct;69(10):2058-2060. doi: 10.2337/dbi20-0031. Diabetes. 2020. PMID: 32958607 Free PMC article. No abstract available.
-
Genetic Associations of Lipids and Lipid-Modifying Drug Targets With Type 2 Diabetes in the Chinese Population.JACC Asia. 2024 Sep 10;4(11):825-838. doi: 10.1016/j.jacasi.2024.07.011. eCollection 2024 Nov. JACC Asia. 2024. PMID: 39619395 Free PMC article.
-
A Mendelian Randomization Approach Using 3-HMG-Coenzyme-A Reductase Gene Variation to Evaluate the Association of Statin-Induced Low-Density Lipoprotein Cholesterol Lowering With Noncardiovascular Disease Phenotypes.JAMA Netw Open. 2021 Jun 1;4(6):e2112820. doi: 10.1001/jamanetworkopen.2021.12820. JAMA Netw Open. 2021. PMID: 34097045 Free PMC article.
-
The Reciprocal Relationship between LDL Metabolism and Type 2 Diabetes Mellitus.Metabolites. 2021 Nov 28;11(12):807. doi: 10.3390/metabo11120807. Metabolites. 2021. PMID: 34940565 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
