

Cardiovascular magnetic resonance in heart transplant patients: diagnostic value of quantitative tissue markers: T2 mapping and extracellular volume fraction, for acute rejection diagnosis
- PMID: 30153847
- PMCID: PMC6114788
- DOI: 10.1186/s12968-018-0480-9
Cardiovascular magnetic resonance in heart transplant patients: diagnostic value of quantitative tissue markers: T2 mapping and extracellular volume fraction, for acute rejection diagnosis
Abstract
Background: The diagnosis of acute rejection in cardiac transplant recipients requires invasive technique with endomyocardial biopsy (EMB) which has risks and limitations. Cardiovascular magnetic resonance imaging (CMR) with T2 and T1 mapping is a promising technique for characterizing myocardial tissue. The purpose of the study was to evaluate T2, T1 and extracellular volume fraction (ECV) quantification as novel tissue markers to diagnose acute rejection.
Methods: CMR was prospectively performed in 20 heart transplant patients providing 31 comparisons EMB-CMR. CMR was performed close to EMB. Images were acquired on a 1.5 Tesla scanner including T2 mapping (T2 prepared balanced steady state free precession) and T1 mapping (modified Look-Locker inversion recovery sequences: MOLLI) at basal, mid and apical level in short axis view. Global and segmental T2 and T1 values were measured before and 15 min (for T1 mapping) after contrast administration.
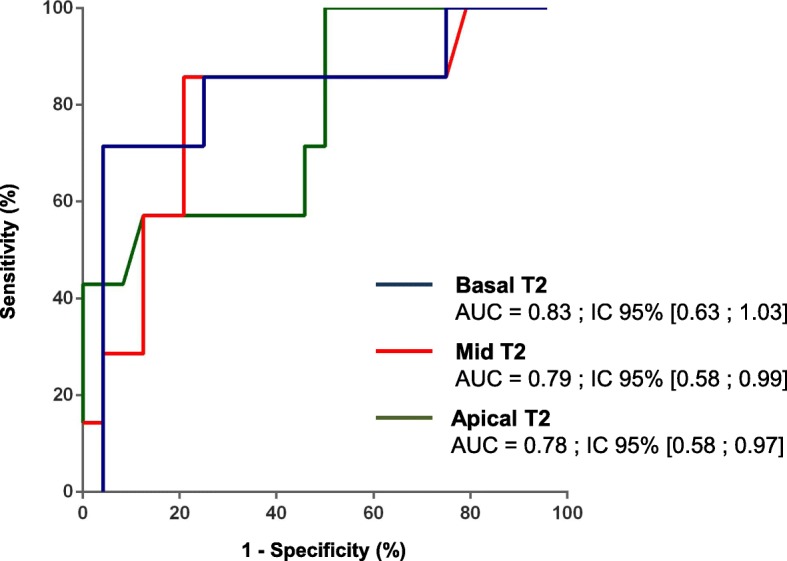
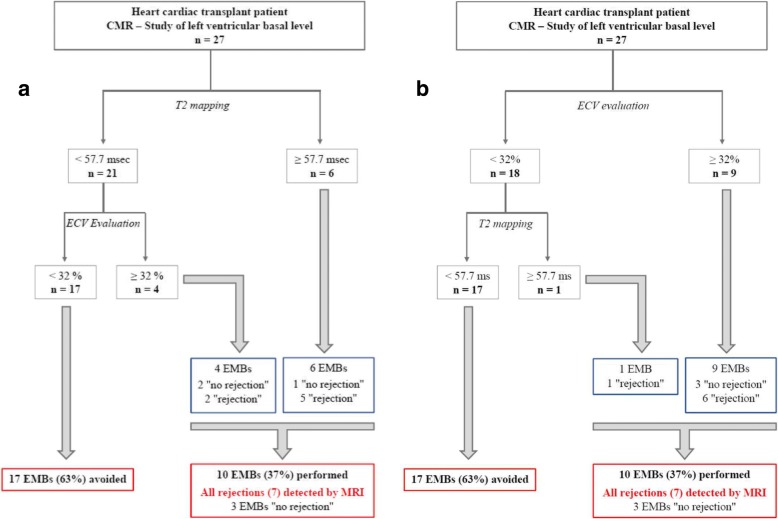
Results: Acute rejection was diagnosed in seven patients: six cellular rejections (4 grade IR, 2 grade 2R) and one antibody mediated rejection. Patients with acute rejection had significantly higher global T2 values at 3 levels: 58.5 ms [55.0-60.3] vs 51.3 ms [49.5-55.2] (p = 0.007) at basal; 55.7 ms [54.0-59.7] vs 51.8 ms [50.1-53.6] (p = 0.002) at median and 58.2 ms [54.0-63.7] vs 53.6 ms [50.8-57.4] (p = 0.026) at apical level. The area under the curve (AUC) for each level was 0.83, 0.79 and 0.78 respectively. Patients with acute rejection had significantly higher ECV at basal level: 34.2% [32.8-37.4] vs 27.4% [24.6-30.6] (p = 0.006). The AUC for basal level was 0.84. The sensitivity, specificity and diagnosis accuracy for basal T2 (cut off: 57.7 ms) were 71, 96 and 90% respectively; and for basal ECV: (cut off 32%) were 86, 85 and 85% respectively. Combining basal T2 and basal ECV allowed diagnosing all acute rejection and avoiding 63% of EMB.
Conclusions: In heart transplant patients, a combined CMR approach using T2 mapping and ECV quantification provides a high diagnostic accuracy for acute rejection diagnosis and could potentially decrease the number of routine EMB.
Keywords: Acute cardiac rejection; Cardiovascular magnetic resonance; Endomyocardial biopsy; T1 and T2 mapping.
Conflict of interest statement
Ethics approval and consent to participate
The local committee named “ethic committee of the cardiovascular department” approved the study.
All patients gave informed written consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Chambers DC, Yusen RD, Cherikh WS, Goldfarb SB, Kucheryavaya AY, Khusch K, et al. The Registry of the International Society for Heart and Lung Transplantation: Thirty-fourth Adult Lung And Heart-Lung Transplantation Report-2017; Focus Theme: Allograft ischemic time. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. 2017;36:1047–59. - PubMed
-
- Kofler S, Bigdeli AK, Kaczmarek I, Kellerer D, Müller T, Schmoeckel M, et al. Long-term outcomes after 1000 heart transplantations in six different eras of innovation in a single center. Transpl Int Off J Eur Soc Organ Transplant. 2009;22:1140–1150. doi: 10.1111/j.1432-2277.2009.00931.x. - DOI - PubMed
-
- Costanzo MR, Dipchand A, Starling R, Anderson A, Chan M, Desai S, et al. The International Society of Heart and Lung Transplantation Guidelines for the care of heart transplant recipients. J Heart Lung Transplant Off Publ Int Soc Heart Transplant. 2010;29:914–956. doi: 10.1016/j.healun.2010.05.034. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
