

Coronary Hemodynamics in Patients With Severe Aortic Stenosis and Coronary Artery Disease Undergoing Transcatheter Aortic Valve Replacement: Implications for Clinical Indices of Coronary Stenosis Severity
- PMID: 30154062
- PMCID: PMC6197079
- DOI: 10.1016/j.jcin.2018.07.019
Coronary Hemodynamics in Patients With Severe Aortic Stenosis and Coronary Artery Disease Undergoing Transcatheter Aortic Valve Replacement: Implications for Clinical Indices of Coronary Stenosis Severity
Abstract
Objectives: In this study, a systematic analysis was conducted of phasic intracoronary pressure and flow velocity in patients with severe aortic stenosis (AS) and coronary artery disease, undergoing transcatheter aortic valve replacement (TAVR), to determine how AS affects: 1) phasic coronary flow; 2) hyperemic coronary flow; and 3) the most common clinically used indices of coronary stenosis severity, instantaneous wave-free ratio and fractional flow reserve.
Background: A significant proportion of patients with severe aortic stenosis (AS) have concomitant coronary artery disease. The effect of the valve on coronary pressure, flow, and the established invasive clinical indices of stenosis severity have not been studied.
Methods: Twenty-eight patients (30 lesions, 50.0% men, mean age 82.1 ± 6.5 years) with severe AS and coronary artery disease were included. Intracoronary pressure and flow assessments were performed at rest and during hyperemia immediately before and after TAVR.
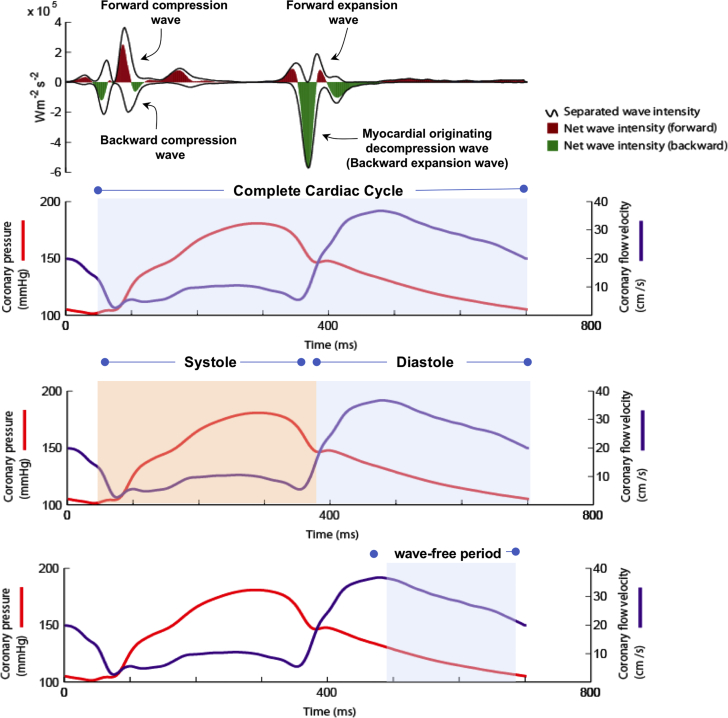
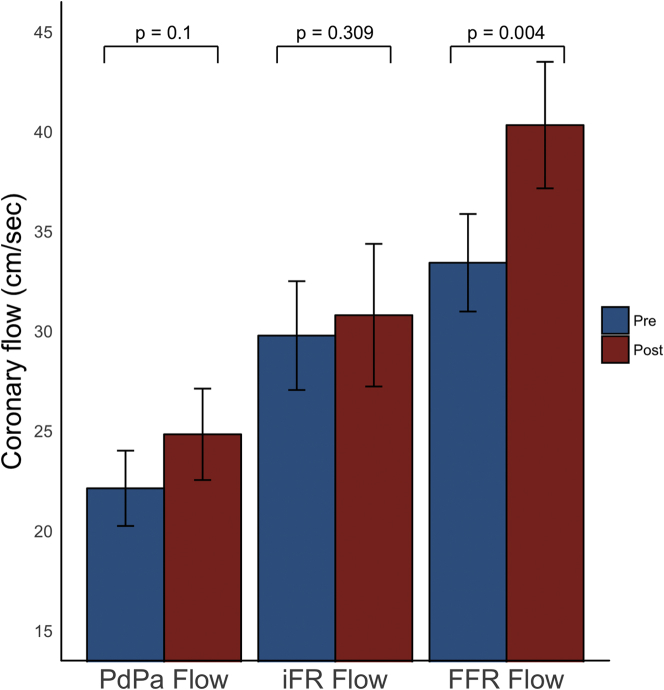
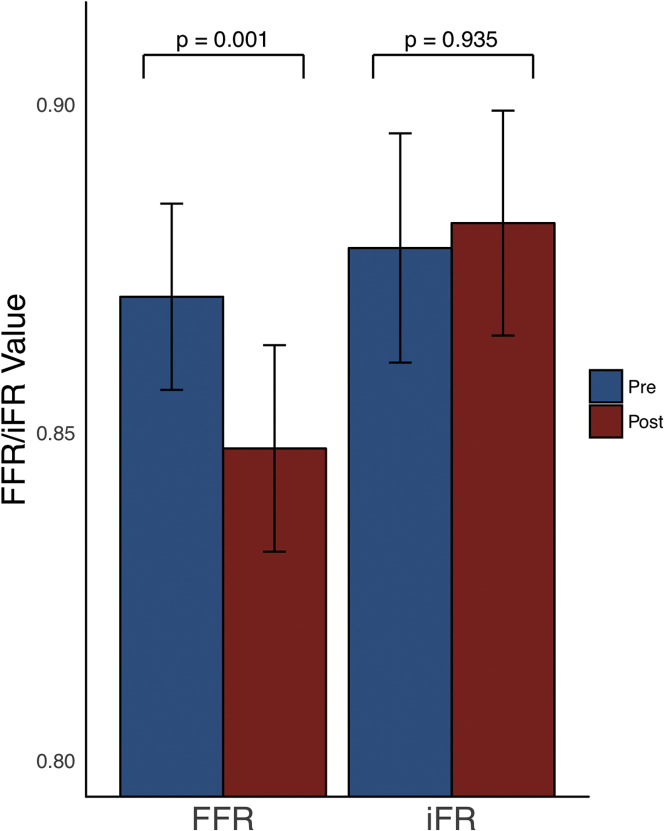
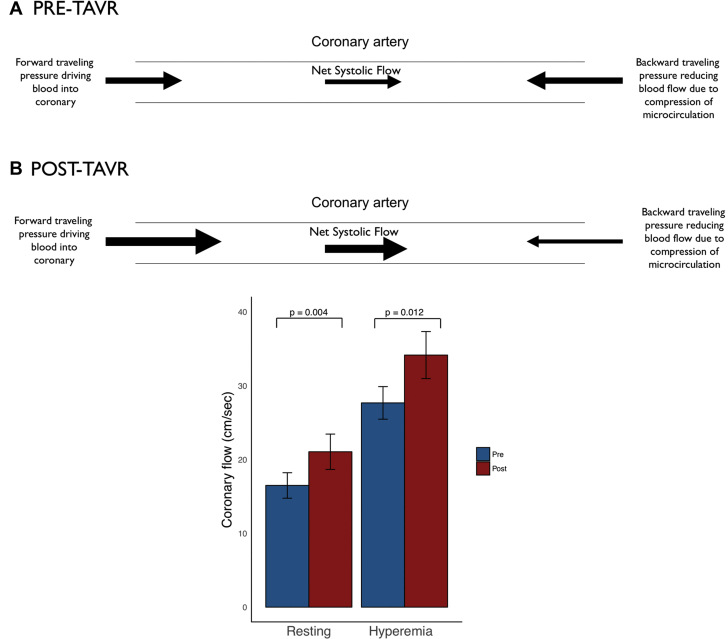
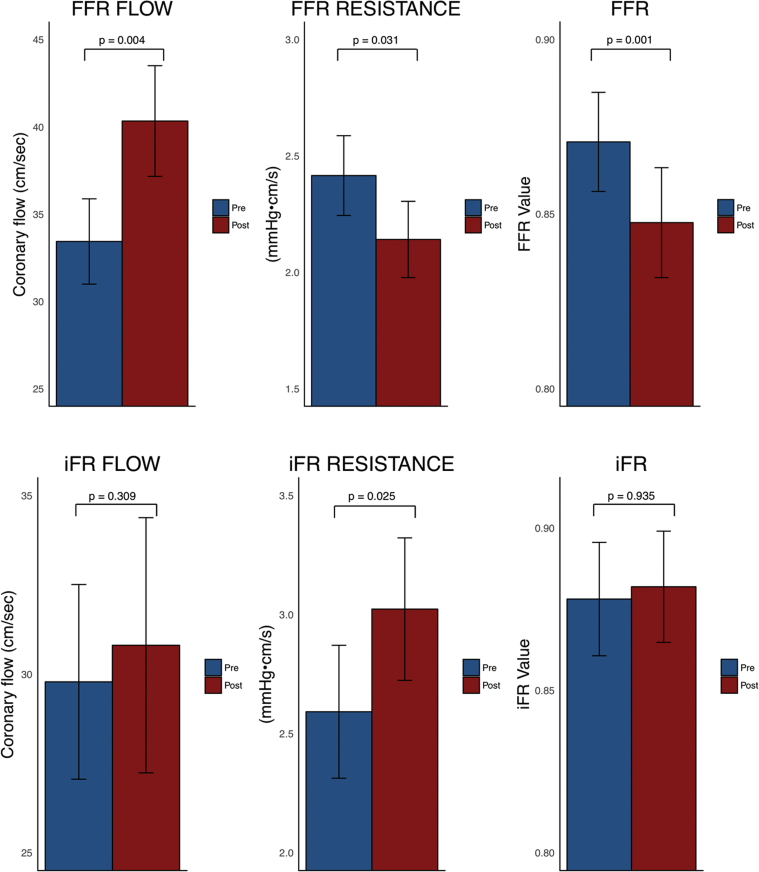
Results: Flow during the wave-free period of diastole did not change post-TAVR (29.78 ± 14.9 cm/s vs. 30.81 ± 19.6 cm/s; p = 0.64). Whole-cycle hyperemic flow increased significantly post-TAVR (33.44 ± 13.4 cm/s pre-TAVR vs. 40.33 ± 17.4 cm/s post-TAVR; p = 0.006); this was secondary to significant increases in systolic hyperemic flow post-TAVR (27.67 ± 12.1 cm/s pre-TAVR vs. 34.15 ± 17.5 cm/s post-TAVR; p = 0.02). Instantaneous wave-free ratio values did not change post-TAVR (0.88 ± 0.09 pre-TAVR vs. 0.88 ± 0.09 post-TAVR; p = 0.73), whereas fractional flow reserve decreased significantly post-TAVR (0.87 ± 0.08 pre-TAVR vs. 0.85 ± 0.09 post-TAVR; p = 0.001).
Conclusions: Systolic and hyperemic coronary flow increased significantly post-TAVR; consequently, hyperemic indices that include systole underestimated coronary stenosis severity in patients with severe AS. Flow during the wave-free period of diastole did not change post-TAVR, suggesting that indices calculated during this period are not vulnerable to the confounding effect of the stenotic aortic valve.
Keywords: TAVR; aortic stenosis; coronary flow; fractional flow reserve; instantaneous wave-free ratio.
Copyright © 2018 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Interface Between Coronary Physiology and Severe Aortic Stenosis: Relax and Go With the Flow.JACC Cardiovasc Interv. 2018 Oct 22;11(20):2041-2043. doi: 10.1016/j.jcin.2018.07.045. Epub 2018 Aug 25. JACC Cardiovasc Interv. 2018. PMID: 30154063 No abstract available.
References
-
- Stewart B.F., Siscovick D., Lind B.K. Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am. Coll Cardiol. 1997;29:630–634. - PubMed
-
- Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC) European Association for Cardio-Thoracic Surgery (EACTS) Vahanian A. Guidelines on the management of valvular heart disease (version 2012) Eur Heart J. 2012;33:2451–2496. - PubMed
-
- Tonino P.A.L., De Bruyne B., Pijls N.H.J. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360:213–224. - PubMed
-
- Pijls N.H., De Bruyne B., Peels K. Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996;334:1703–1708. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
