

The relationship between sex hormones, the vaginal microbiome and immunity in HIV-1 susceptibility in women
- PMID: 30154116
- PMCID: PMC6177003
- DOI: 10.1242/dmm.035147
The relationship between sex hormones, the vaginal microbiome and immunity in HIV-1 susceptibility in women
Abstract
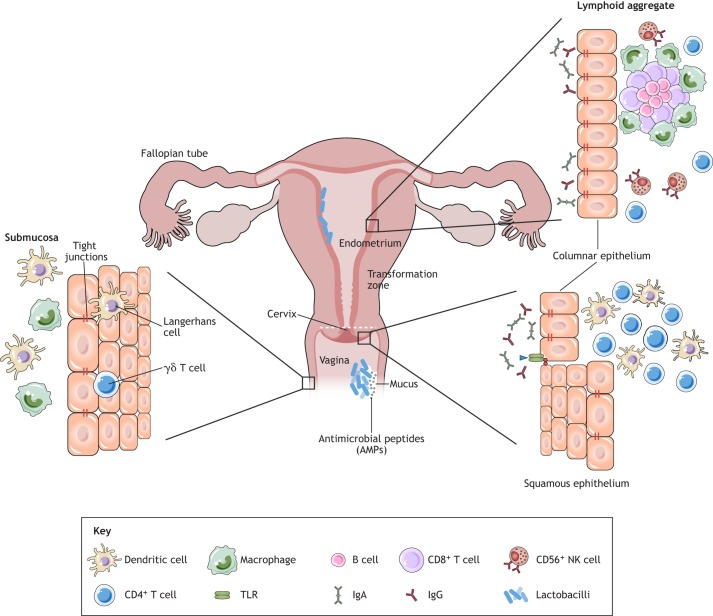
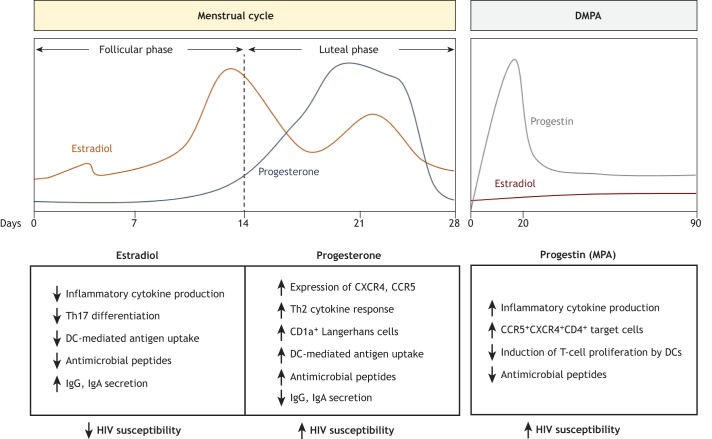
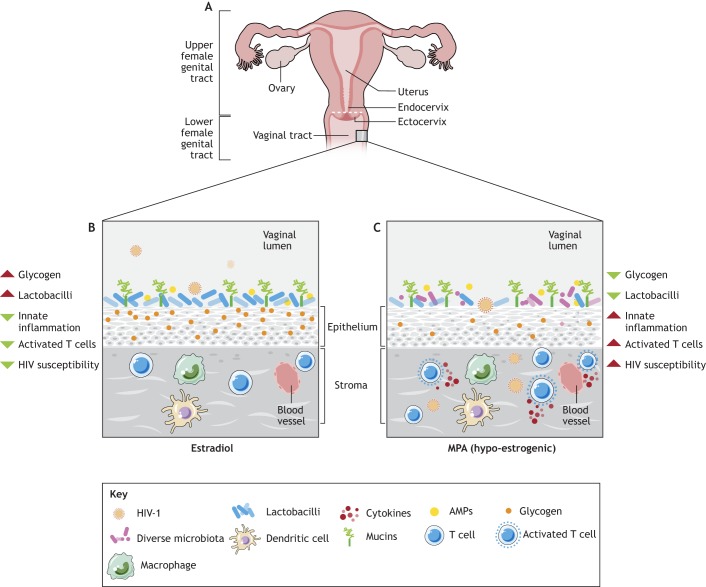
The role of sex hormones in regulating immune responses in the female genital tract has been recognized for decades. More recently, it has become increasingly clear that sex hormones regulate susceptibility to sexually transmitted infections through direct and indirect mechanisms involving inflammation and immune responses. The reproductive cycle can influence simian/human immunodeficiency virus (SHIV) infections in primates and HIV-1 infection in ex vivo cervical tissues from women. Exogenous hormones, such as those found in hormonal contraceptives, have come under intense scrutiny because of the increased susceptibility to sexually transmitted infections seen in women using medroxyprogesterone acetate, a synthetic progestin-based contraceptive. Recent meta-analyses concluded that medroxyprogesterone acetate enhanced HIV-1 susceptibility in women by 40%. In contrast, estradiol-containing hormonal contraceptives were not associated with increased susceptibility and some studies reported a protective effect of estrogen on HIV/SIV infection, although the underlying mechanisms remain incompletely understood. Recent studies describe a key role for the vaginal microbiota in determining susceptibility to sexually transmitted infections, including HIV-1. While Lactobacillus spp.-dominated vaginal microbiota is associated with decreased susceptibility, complex microbiota, such as those seen in bacterial vaginosis, correlates with increased susceptibility to HIV-1. Interestingly, sex hormones are inherently linked to microbiota regulation in the vaginal tract. Estrogen has been postulated to play a key role in establishing a Lactobacillus-dominated microenvironment, whereas medroxyprogesterone acetate is linked to hypo-estrogenic effects. The aim of this Review is to contribute to a better understanding of the sex-hormone-microbiome-immunity axis, which can provide key information on the determinants of HIV-1 susceptibility in the female genital tract and, consequently, inform HIV-1 prevention strategies.
Keywords: DMPA; Inflammation; T cells; Vaginal microbiota.
© 2018. Published by The Company of Biologists Ltd.
Conflict of interest statement
Competing interestsThe authors declare no competing or financial interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
