

Evaluating intrinsic and non-intrinsic cancer risk factors
- PMID: 30154431
- PMCID: PMC6113228
- DOI: 10.1038/s41467-018-05467-z
Evaluating intrinsic and non-intrinsic cancer risk factors
Abstract
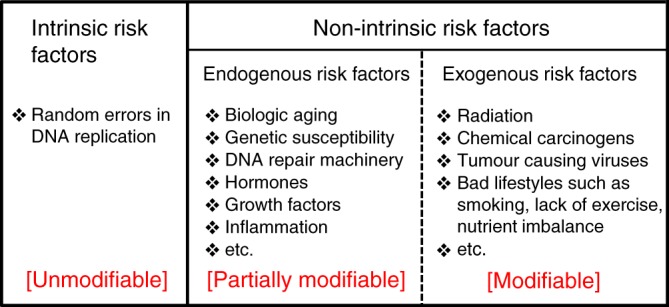
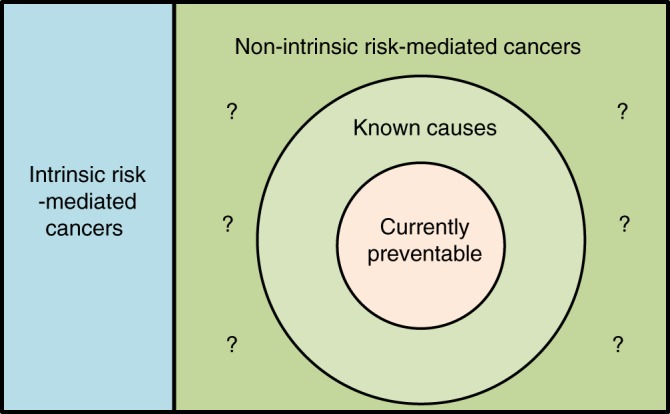
Discriminating the contribution of unmodifiable random intrinsic DNA replication errors ('bad luck') to cancer development from those of other factors is critical for understanding cancer in humans and for directing public resources aimed at reducing the burden of cancer. Here, we review and highlight the evidence that demonstrates cancer causation is multifactorial, and provide several important examples where modification of risk factors has achieved cancer prevention. Furthermore, we stress the need and opportunities to advance understanding of cancer aetiology through integration of interaction effects between risk factors when estimating the contribution of individual and joint factors to cancer burden in a population. We posit that non-intrinsic factors drive most cancer risk, and stress the need for cancer prevention.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
