

A prospective study of screening for musculoskeletal pathology in the child with a limp or pseudoparalysis using erythrocyte sedimentation rate, C-reactive protein and MRI
- PMID: 30154932
- PMCID: PMC6090194
- DOI: 10.1302/1863-2548.12.180004
A prospective study of screening for musculoskeletal pathology in the child with a limp or pseudoparalysis using erythrocyte sedimentation rate, C-reactive protein and MRI
Abstract
Purpose: To determine if the detection of musculoskeletal pathology in children with a limp or acute limb disuse can be optimized by screening with blood tests for raised inflammatory markers, followed by MRI.
Methods: This was a prospective observational study. Entry criteria were children (0 to 16 years of age) presenting to our emergency department with a non-traumatic limp or pseudoparalysis of a limb, and no abnormality on plain radiographs. Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) blood tests were performed. Children with ESR > 10 mm/hr or CRP > 10 mg/L underwent a MRI scan. When the location of the pathology causing the limp was clinically unclear, screening images (Cor t1 and Short Tau Inversion Recovery) of both lower limbs from pelvis to ankles ('legogram') was undertaken. Data was gathered prospectively from 100 consecutive children meeting the study criteria.
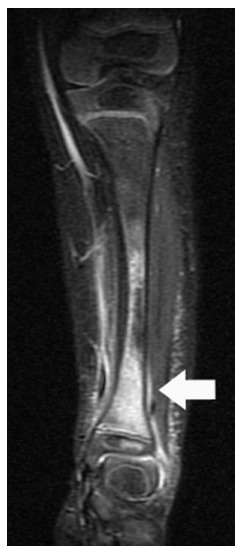
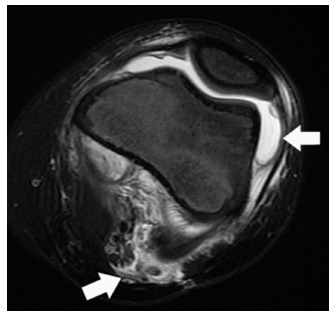
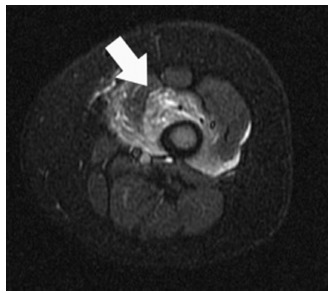
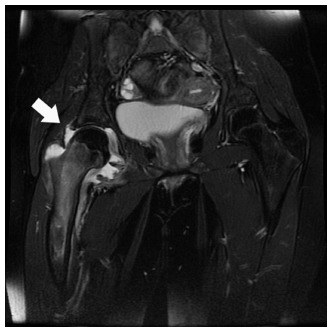
Results: In all, 75% of children had a positive finding on their MRI. A total of 64% of cases had an infective cause for their symptoms (osteomyelitis, septic arthritis, pyomyositis, fasciitis, cellulitis or discitis). A further 11% had positive findings on MRI from non-infective causes (juvenile idiopathic arthritis, cancer or undisplaced fracture). The remaining 25% had either a normal scan or effusion due to transient synovitis. ESR was a more sensitive marker than CRP in infection, since ESR was raised in 97%, but CRP in only 70%.
Conclusion: In our opinion MRI imaging of all children with a limp and either raised ESR or CRP is a sensitive method to minimize the chance of missing important pathology in this group, and is an effective use of MRI resources. We advocate the use of both blood tests in conjunction.
Level of evidence: Level II.
Keywords: cancer; juvenile idiopathic arthritis; osteomyelitis; pyomyositis; septic arthritis.
Figures
Similar articles
-
Managing children with acute non-traumatic limp: the utility of clinical findings, laboratory inflammatory markers and X-rays.Emerg Med Australas. 2009 Apr;21(2):136-42. doi: 10.1111/j.1742-6723.2008.01144.x. Emerg Med Australas. 2009. PMID: 19422411
-
Epidemiology, diagnosis, and treatment of pericapsular pyomyositis of the hip in children.J Pediatr Orthop. 2014 Apr-May;34(3):316-25. doi: 10.1097/BPO.0000000000000106. J Pediatr Orthop. 2014. PMID: 24172679
-
Distinguishing Pediatric Lyme Arthritis of the Hip from Transient Synovitis and Acute Bacterial Septic Arthritis: A Systematic Review and Meta-analysis.Cureus. 2018 Jan 25;10(1):e2112. doi: 10.7759/cureus.2112. Cureus. 2018. PMID: 29581924 Free PMC article.
-
Test characteristics of history, examination and investigations in the evaluation for septic arthritis in the child presenting with acute non-traumatic limp. A systematic review.BMJ Open. 2020 Dec 30;10(12):e038088. doi: 10.1136/bmjopen-2020-038088. BMJ Open. 2020. PMID: 33380476 Free PMC article.
-
Bone and Joint Infections in Children: Septic Arthritis.Indian J Pediatr. 2016 Aug;83(8):825-33. doi: 10.1007/s12098-015-1816-1. Epub 2015 Jul 21. Indian J Pediatr. 2016. PMID: 26189923 Review.
Cited by
-
Acute Flaccid Paralysis in a Child: It Is Not Guillain-Barré Syndrome Always!Indian Pediatr. 2021 Jan 15;58(1):93-94. doi: 10.1007/s13312-021-2115-8. Indian Pediatr. 2021. PMID: 33452794 Free PMC article. No abstract available.
References
-
- Sawyer JR, Kapoor M. The limping child: a systematic approach to diagnosis. Am Fam Physician 2009;79:215–224. - PubMed
-
- Perry DC, Bruce C. Evaluating the child who presents with an acute limp. BMJ 2010;341:c4250. - PubMed
-
- Herman MJ, Martinek M. The limping child. Pediatr Rev 2015;36:184–195. - PubMed
-
- Naranje S, Kelly DM, Sawyer JR. A systematic approach to the evaluation of a limping child. Am Fam Physician 2015;92:908–916. - PubMed
-
- Do TT. Transient synovitis as a cause of painful limps in children. Curr Opin Pediatr 2000;12:48–51. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
