

Case Report and Literature Review Illustrating the Clinical, Endoscopic, Radiologic, and Histopathologic Findings with Prepouch Ileitis after IPAA and Restorative Proctocolectomy for Refractory Ulcerative Colitis
- PMID: 30155319
- PMCID: PMC6091410
- DOI: 10.1155/2018/7506069
Case Report and Literature Review Illustrating the Clinical, Endoscopic, Radiologic, and Histopathologic Findings with Prepouch Ileitis after IPAA and Restorative Proctocolectomy for Refractory Ulcerative Colitis
Abstract
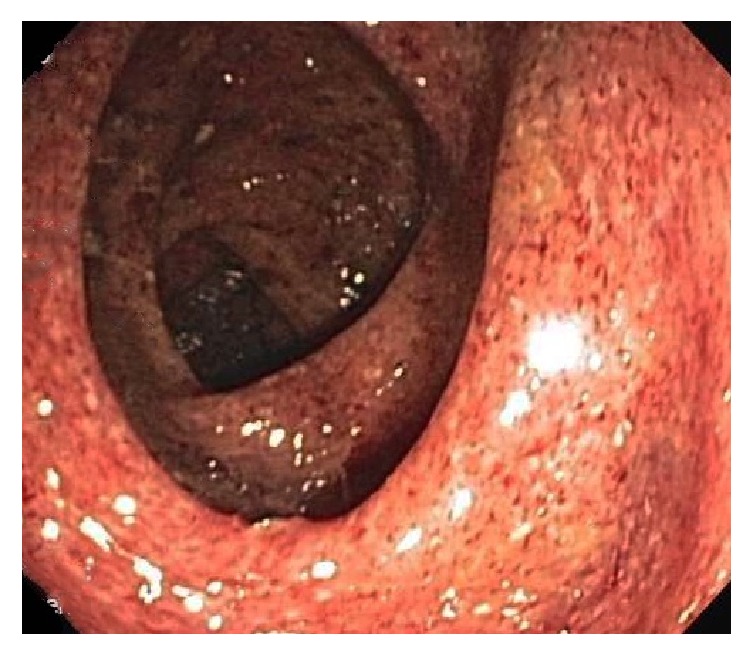
Prepouch ileitis (PI) is an uncommon complication of ileal pouch anal anastomosis (IPAA) and restorative proctocolectomy (RPC) for treatment of refractory ulcerative colitis (UC). A case is reported of PI in a 16-year-old girl who presented with severe UC that was initially stabilized with infliximab therapy but re-presented 1 year later with severe UC, refractory to infliximab and corticosteroid therapy, which required IPAA and RPC. Her symptoms resolved postoperatively, but she re-presented 1 year later with 10 loose, bloody, bowel movements/day and involuntary 6-Kg weight-loss. Computerized tomographic enterography showed focal narrowing and mucosal enhancement of the pouch and focal narrowing, abnormal mucosal enhancement, and mural thickening of the prepouch ileum. Pouchoscopy revealed exudates and ulcerations in both the pouch and prepouch ileum up to 50 cm proximal to pouch, as confirmed by histopathology of pouch and ileal biopsies. Capsule endoscopy revealed no small intestinal lesions beyond 50 cm from the pouch. She required antibiotics, hydrocortisone enemas, and eventually azathioprine to control her symptoms. She remains asymptomatic 4 years later while chronically administered azathioprine therapy. Comprehensive literature review demonstrates that this case illustrates the classical clinical, radiologic, endoscopic, and histopathologic findings in PI, a relatively rare syndrome.
Figures




References
-
- Shen B., Bennett A. E., Navaneethan U., et al. Primary sclerosing cholangitis is associated with endoscopic and histologic inflammation of the distal afferent limb in patients with ileal pouch-anal anastomosis. Inflammatory Bowel Diseases. 2011;17(9):1890–1900. doi: 10.1002/ibd.21594. - DOI - PubMed
-
- McLaughlin S. D., Clark S. K., Bell A. J., Tekkis P. P., Ciclitira P. J., Nicholls R. J. Incidence and short-term implications of prepouch ileitis following restorative proctocolectomy with ileal pouch-anal anastomosis for ulcerative colitis. Diseases of the Colon & Rectum. 2009;52(5):879–883. doi: 10.1007/DCR.0b013e3181a4f9fa. - DOI - PubMed
-
- Mclaughlin S. D., Clark S. K., Bell A. J., Tekkis P. P., Ciclitira P. J., Nicholls R. J. An open study of antibiotics for the treatment of pre-pouch ileitis following restorative proctocolectomy with ileal pouch-anal anastomosis. Alimentary Pharmacology & Therapeutics. 2009;29(1):69–74. doi: 10.1111/j.1365-2036.2008.03858.x. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
