

Long-term survival and related outcomes for hybrid versus traditional arch repair-a meta-analysis
- PMID: 30155410
- PMCID: PMC6094005
- DOI: 10.21037/acs.2018.05.07
Long-term survival and related outcomes for hybrid versus traditional arch repair-a meta-analysis
Abstract
Background: Surgical interventions for aortic aneurysm and dissection remain associated with high risk of mortality and morbidity. Advances in operative techniques have led to a variety of options for the cardiac surgeon, including endovascular and hybrid approaches. Debate remains over which of these techniques provide optimal outcomes for the patient. The present systematic review and meta-analysis aims to evaluate long term patient survival and identify short-term outcomes for conventional (open) aortic arch repair and hybrid aortic arch repair (HAR).
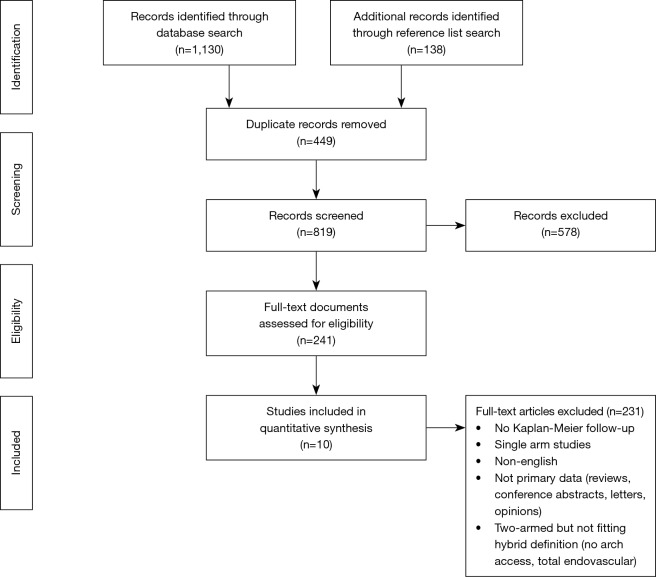
Methods: An electronic literature search was conducted according to predefined inclusion criteria for hybrid and conventional aortic arch repair surgery. Digitized survival data was extracted from identified studies' Kaplan-Meier curves and used to re-create individual patient data for aggregated survival analysis. Post-operative morbidity and mortality were analyzed using random-effects model meta-analysis.
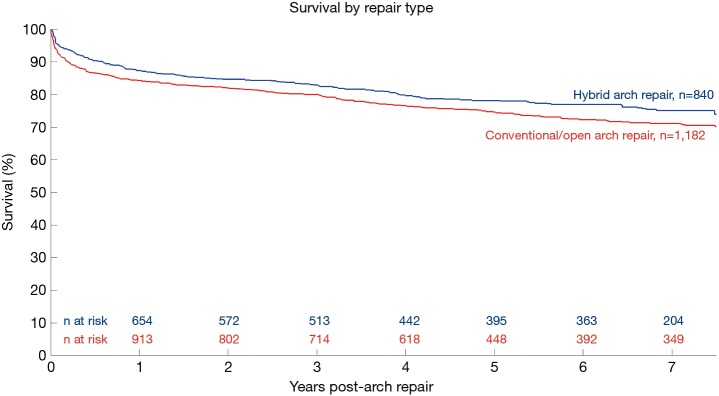
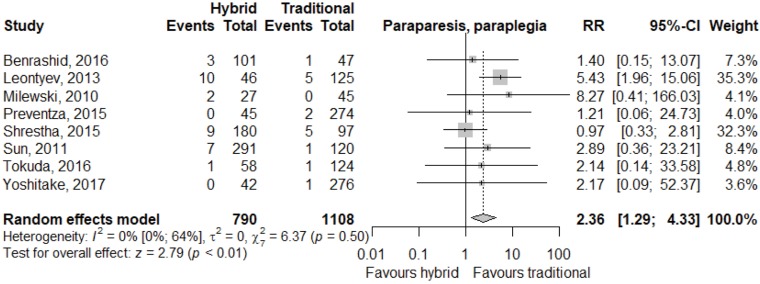
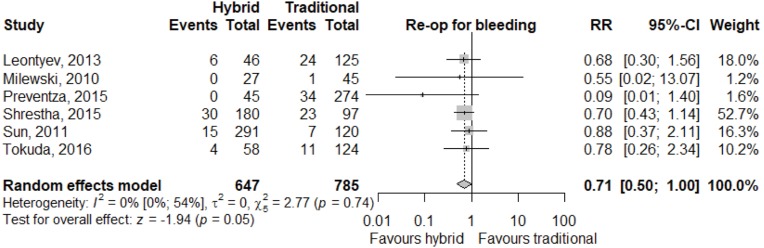
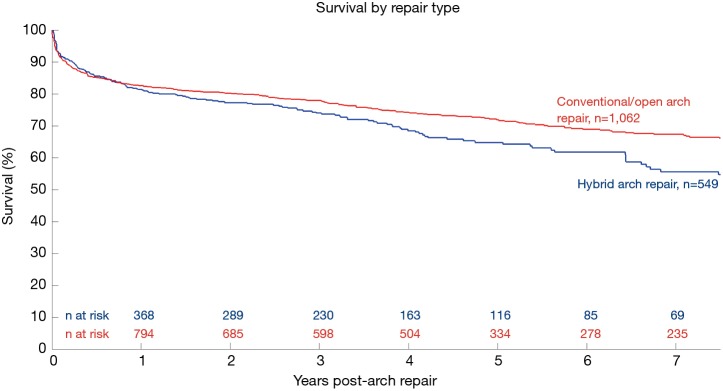
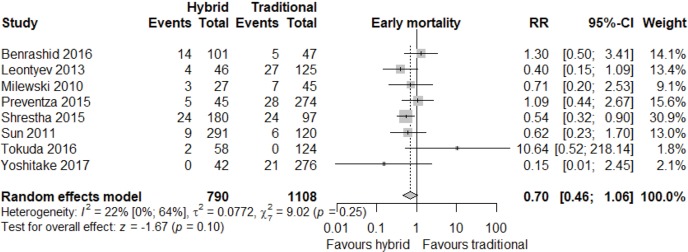
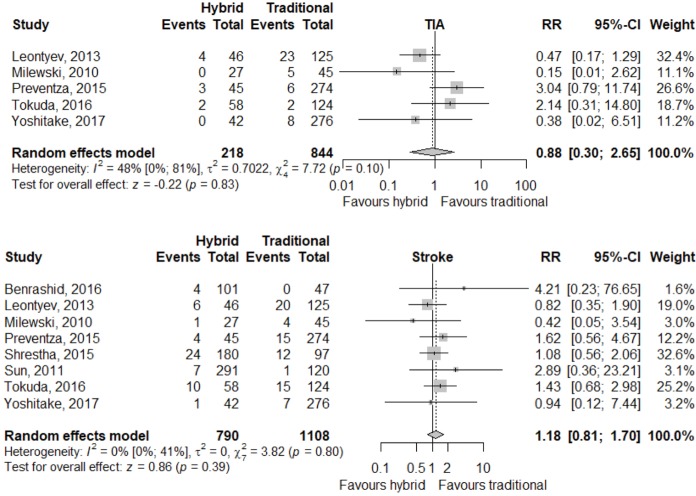
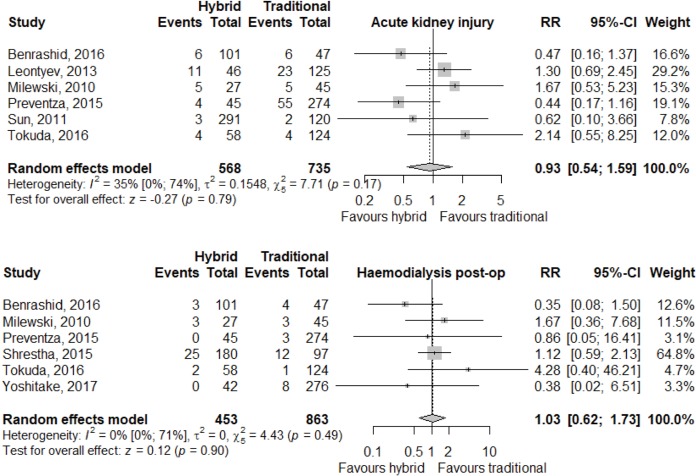
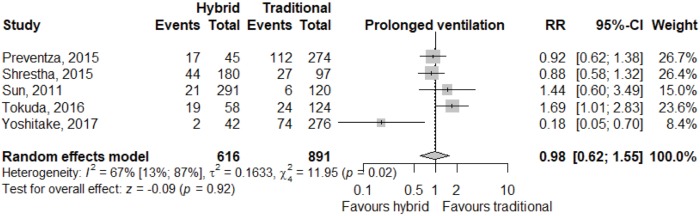
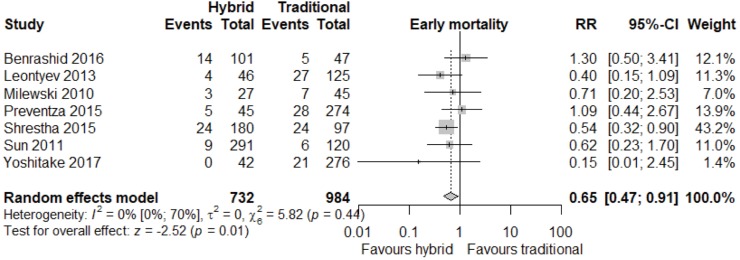
Results: Nine studies were included, containing 841 hybrid arch repair and 1,182 conventional arch repair patients. Pooled Kaplan-Meier analysis of all patients demonstrated higher survival in hybrid arch repair patients than conventional arch repair patients, however, this was noted to be sensitive to results from a particular study. Overall results showed for the hybrid repair cohort, survival at 1, 2, 3, 5 and 7 years was 87%, 85%, 83%, 78% and 75%, respectively. Survival in the conventional repair cohort at 1, 2, 3, 5 and 7 years was 84%, 82%, 80%, 75% and 71%, respectively. Statistically significant findings from meta-analysis showed hybrid arch repair was associated with lower risk of re-operation for bleeding, while conventional arch repair was associated with reduced risk of spinal cord injury.
Conclusions: Pooled Kaplan-Meier analysis of all studies showed long-term survival outcomes for hybrid and conventional aortic arch repair patients are heterogeneous and sensitive to the results of particular studies. Superior results from particular centres and the low number of comparative studies mean that more data is required to make definitive findings with regards to the long-term survival outcomes of either procedure. Hybrid arch repair was associated with lower risk of re-operation for bleeding, while conventional arch repair was associated with lower risk of spinal cord injury. Surgeons should consider their own center's experience and patient suitability when deciding between hybrid or conventional aortic repair techniques.
Keywords: Open surgical repair; aortic arch aneurysm; aortic arch replacement; elephant trunk; hybrid arch repair (HAR).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Boening A, Karck M, Conzelmann L, et al. German registry for acute aortic dissection type A: structure, results, and future perspectives. Thorac Cardiovasc Surg 2017;65:077-84. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous