

Editorial
doi: 10.21037/acs.2018.05.06.
Classic hybrid arch debranching (type I hybrid arch repair) without circulatory arrest
Affiliations
- PMID: 30155426
- PMCID: PMC6094021
- DOI: 10.21037/acs.2018.05.06
Item in Clipboard
Editorial
Classic hybrid arch debranching (type I hybrid arch repair) without circulatory arrest
Ann Cardiothorac Surg.
2018 May.
No abstract available
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures

Preoperative 3D (A) and sagittal reconstructed (B) CTA images demonstrating >8 cm diameter aneurysm of the distal aortic arch and proximal descending thoracic aorta secondary to chronic residual dissection after prior hemi-arch repair of acute type A dissection. CTA, computed tomography angiography.

Centerline reconstruction CTA images (A-C) demonstrate >5 cm of potential Dacron proximal landing zone above the proposed inflow site of an arch debranching graft (A). The proximal landing zone within the existing ascending aortic Dacron graft mean diameter was 32 mm (D) and the distal landing zone in the true lumen at the celiac axis measured 21 mm (E). CTA, computed tomography angiography; LCCA, left common carotid artery; LSCA, left subclavian artery.

Intraoperative photographs demonstrating incision sites for type I HAR. If only the innominate and LCCA are to be re-implanted then the incision is typically extended cephalad along the right sternocleidomastoid muscle (A), whereas the incision is typically extended to the left if all three arch vessels are to be re-implanted from the front (B). HAR, hybrid arch repair; LCCA, left common carotid artery.

Intraoperative photograph from the case presented in the clinical vignette demonstrating the proximal end of the ascending aortic Dacron graft mobilized down to the sinotubular junction (STJ) to allow partial clamp placement and create maximal PLZ length. The three arch vessels have been fully mobilized and a vessel loop is seen encircling the left innominate vein. Downward tension on this vessel loop during the arch debranching distal anastomoses facilitates exposure of the arch vessels. LCCA, left common carotid artery; LSCA, left subclavian artery; PLZ, proximal landing zone.

Photograph of commercially available trifurcated woven Dacron graft used for arch debranching. The graft is available with 14- and 12-mm main body sizes with 8-mm limbs, and the graft size is chosen to best match the diameter of the innominate artery.

Intraoperative photograph from another patient undergoing type I HAR after prior type A dissection repair demonstrating the completed proximal anastomosis and reinforcing sutures of pledgeted 4-0 Prolene. A ruler demonstrates the creation of nearly 5 cm of Dacron PLZ in this case. HAR, hybrid arch repair; PLZ, proximal landing zone.

Intraoperative photograph from the case presented in the clinical vignette demonstrating completed proximal anastomosis and radiographic markers placed around the debranching graft origin to facilitate its identification under fluoroscopy.
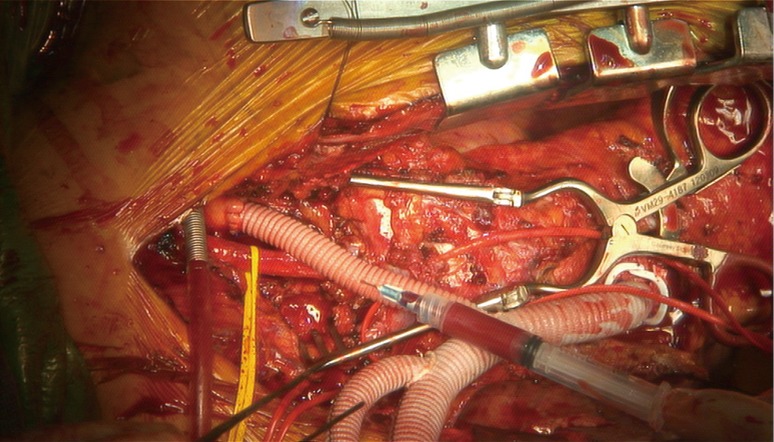
Intraoperative photograph from the case presented in the clinical vignette demonstrating completed distal anastomosis to the LSCA with the graft limb being carefully de-aired using a 25-gauge needle. The graft limb is also de-aired extensively prior to re-establishing antegrade flow via temporary release of the distal clamp on the LSCA prior to tying the suture knots. The importance of careful graft de-airing cannot be over emphasized to avoid cerebral embolization. LSCA, left subclavian artery.

Intraoperative photograph from the same patient as shown in Figure 7 and in whom only the LCCA and innominate artery were re-implanted. The photo in (A) shows the proximal LCCA being stapled with a vascular stapler prior to applying a clamp on the distal LCCA and dividing it above the staple line. The completed anastomosis to the LCCA is shown in (B). LCCA, left common carotid artery.

Drawing of a native zone 0 type I HAR in which LCCA to LSCA bypass has been performed prior to arch debranching. The LCCA-LSCA bypass will provide flow to the LCCA distribution during LCCA debranching and therefore a test clamp is not needed in this setting as the LCCA distribution will not be ischemic. HAR, hybrid arch repair; LSCA, left subclavian artery; LCCA, left common carotid artery.

Intraoperative photograph from the same patient as shown in Figures 6,9 demonstrating the innominate artery being stapled proximally at its origin from the aorta with a vascular stapler (A). The innominate artery is then clamped distally and divided above the staple line (B). The innominate distribution is perfused via the right axillary side graft during this period to a target right radial arterial line pressure of 70 mmHg such that the innominate distribution is not ischemic during the period of debranching. The patient has otherwise been weaned from CPB at this point with the heart ejecting and the lungs ventilated such that the left brain and body are perfused via the native circulation. CPB, cardiopulmonary bypass.

Intraoperative photograph from the case presented in the clinical vignette demonstrating completed stage I arch debranching procedure.

Classic hybrid arch debranching (type I hybrid arch repair) without circulatory arrest.
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources