

Markers of Local Inflammation and Bone Resorption in the Acute Diabetic Charcot Foot
- PMID: 30155488
- PMCID: PMC6098852
- DOI: 10.1155/2018/5647981
Markers of Local Inflammation and Bone Resorption in the Acute Diabetic Charcot Foot
Abstract
Objective: Due to the localized nature of Charcot foot, systemically altered levels of inflammation markers can be difficult to measure. The aim of this study was to investigate whether it is possible to detect an arteriovenous (A-V) flux in any locally produced inflammatory biomarkers from an acute Charcot foot by comparing local and systemic measurements.
Methods: We included patients with acute diabetic Charcot foot. Blood was sampled from the vena saphena magna on the distal part of the crus bilaterally as well as from the arteria radialis. To minimize the A-V shunting effect, the feet were externally cooled with ice water prior to resampling.
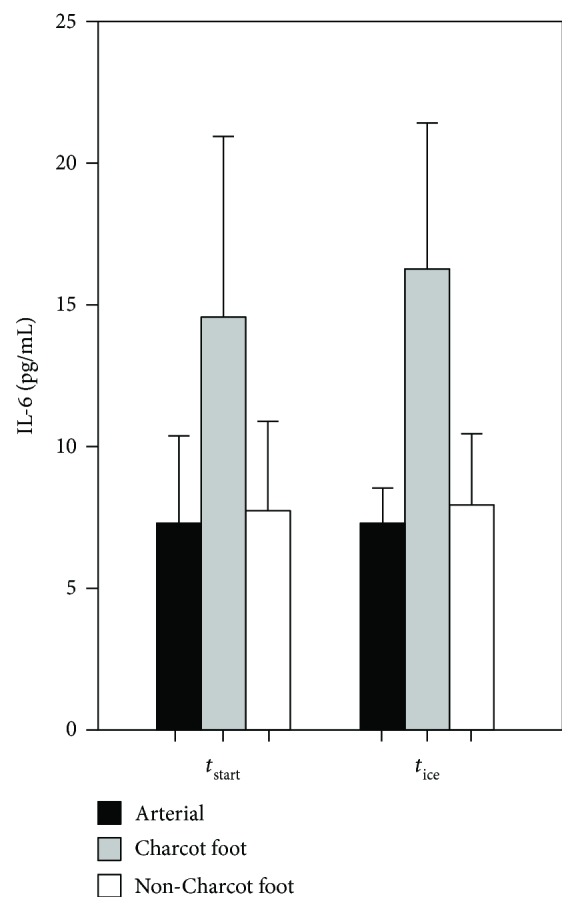
Results: Both before and after cooling, the A-V flux of interleukin-6 (IL-6) between the Charcot feet and the arterial level was significantly higher than the flux between the healthy feet and the arterial level (Δvaluebefore: 7.25 versus 0.41 pg/mL, resp., p = 0.008; Δvalueafter: 10.04 versus 1.68 pg/mL, resp., p = 0.032). There were no differences in the fluxes for other markers of inflammation.
Conclusion: We have found an increased A-V flux of IL-6 in the acute diabetic Charcot foot compared to the healthy foot in the same patients.
Figures

References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
