

Acute kidney injury in neonatal encephalopathy: an evaluation of the AWAKEN database
- PMID: 30155763
- PMCID: PMC6986688
- DOI: 10.1007/s00467-018-4068-2
Acute kidney injury in neonatal encephalopathy: an evaluation of the AWAKEN database
Erratum in
-
Correction to: Acute kidney injury in neonatal encephalopathy: an evaluation of the AWAKEN database.Pediatr Nephrol. 2019 Feb;34(2):363. doi: 10.1007/s00467-018-4106-0. Pediatr Nephrol. 2019. PMID: 30315405
Abstract
Background: Acute kidney injury (AKI) is common in neonatal encephalopathy (NE) and is associated with worse outcomes. Our objectives were to determine the incidence, risk factors, and outcomes of AKI in infants with NE.
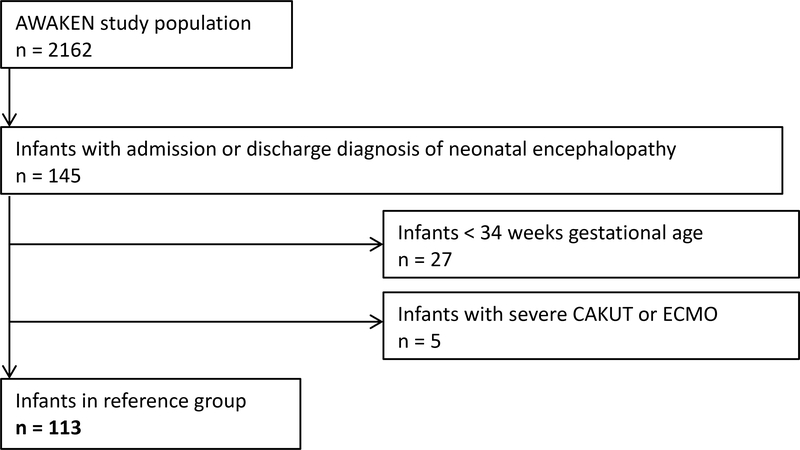
Methods: We performed a retrospective analysis of infants ≥ 34 weeks' gestational age with a diagnosis of NE from the Analysis of Worldwide Acute Kidney injury Epidemiology in Neonates (AWAKEN) database. AKI was defined using the modified Kidney Disease Improving Global Outcomes criteria. Perinatal and postnatal factors were evaluated. Multivariate logistic and linear regressions were performed.
Results: One hundred and thirteen patients with NE were included. 41.6% (47) developed AKI. Being born outside the admitting institution (OR 4.3; 95% CI 1.2-14.8; p = 0.02), intrauterine growth restriction (OR 10.3, 95% CI 1.1-100.5; p = 0.04), and meconium at delivery (OR 2.8, 95% CI 1.04-7.7; p = 0.04) conferred increased odds of AKI. After controlling for confounders, infants with AKI stayed in the hospital an average of 8.5 days longer than infants without AKI (95% CI 0.79-16.2 days; p = 0.03).
Conclusions: In this multi-national analysis, several important perinatal factors were associated with AKI and infants with both NE and AKI had longer length of stay than NE alone. Future research aimed at early AKI detection, renoprotective management strategies, and understanding the long-term renal consequences is warranted in this high-risk group of patients.
Keywords: Acute kidney injury; Hypoxic-ischemic encephalopathy; Neonatal encephalopathy; Neonate.
Conflict of interest statement
Conflict of interest disclosures
All authors declare no real or perceived conflicts of interest that could affect the study design, collection, analysis and interpretation of data, writing of the report, or the decision to submit for publication.
For full disclosure, we provide here an additional list of other author’s commitments and funding sources that are not directly related to this study: David J Askenazi serves on the speaker board for Baxter (Baxter, USA), and the Acute Kidney Injury (AKI) Foundation (Cincinnati, OH, USA); he also receives grant funding for studies not related to this manuscript from National Institutes of Health — National Institutes of Diabetes and Digestive and Kidney Diseases (NIH-NIDDK, R01 DK103608 and NIH-FDA (R01 FD005092). Danielle E. Soranno also receives grant funding for studies not related to this manuscript from National Institutes of Health - National Institute of Diabetes and Digestive and Kidney Diseases, 1K08DK109226-01A1.
Figures
References
-
- Pfister RH, Soll RF. Hypothermia for the treatment of infants with hypoxic-ischemic encephalopathy. J Perinatol. 2010;30 Suppl:S82–7. - PubMed
-
- Karlowicz MG, Adelman RD. Nonoliguric and oliguric acute renal failure in asphyxiated term neonates. Pediatr Nephrol. 1995;9(6):718–22. - PubMed
-
- Gupta BD, Sharma P, Bagla J, Parakh M, Soni JP. Renal failure in asphyxiated neonates. Indian Pediatr. 2005;42(9):928–34. - PubMed
-
- Carmody JB, Charlton JR. Short-term gestation, long-term risk: prematurity and chronic kidney disease. Pediatrics. 2013;131(6):1168–79. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
