

Phase II study of ERC1671 plus bevacizumab versus bevacizumab plus placebo in recurrent glioblastoma: interim results and correlations with CD4+ T-lymphocyte counts
- PMID: 30157683
- PMCID: PMC6200061
- DOI: 10.2217/cns-2018-0009
Phase II study of ERC1671 plus bevacizumab versus bevacizumab plus placebo in recurrent glioblastoma: interim results and correlations with CD4+ T-lymphocyte counts
Abstract
Aim: ERC1671 is an allogeneic/autologous therapeutic glioblastoma (GBM) vaccine - composed of whole, inactivated tumor cells mixed with tumor cell lysates derived from the patient and three GBM donors.
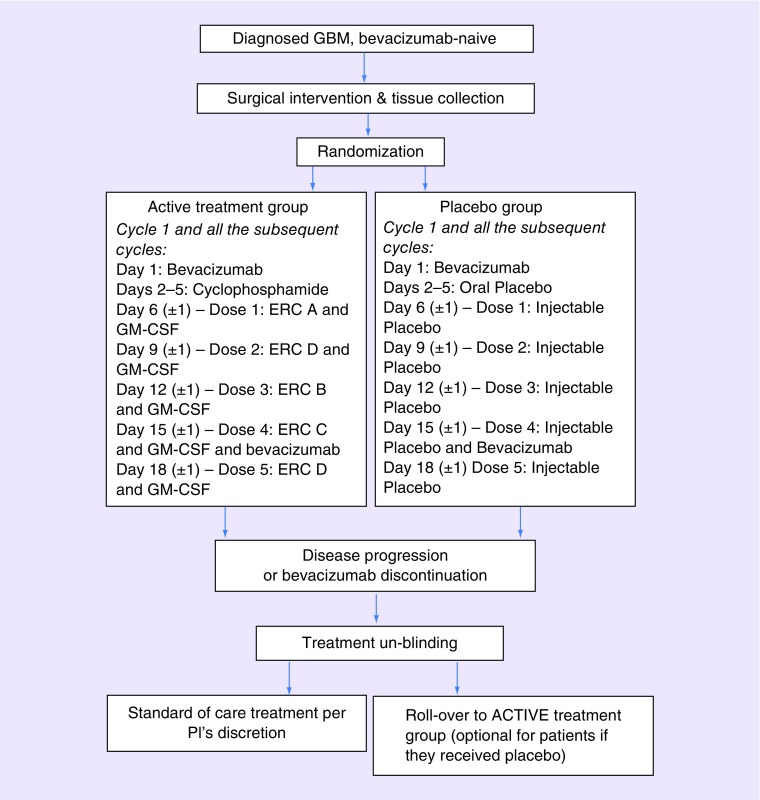
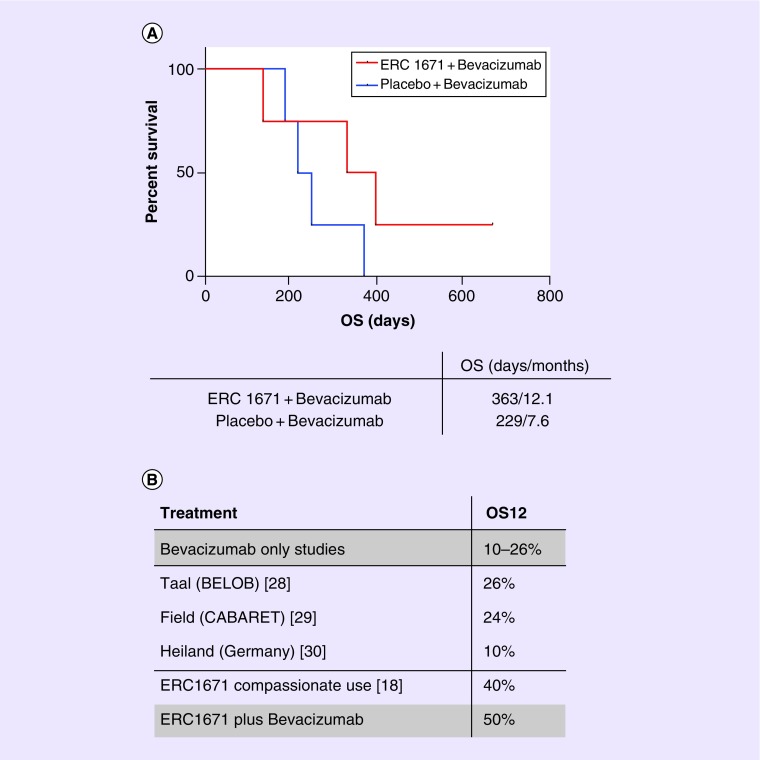
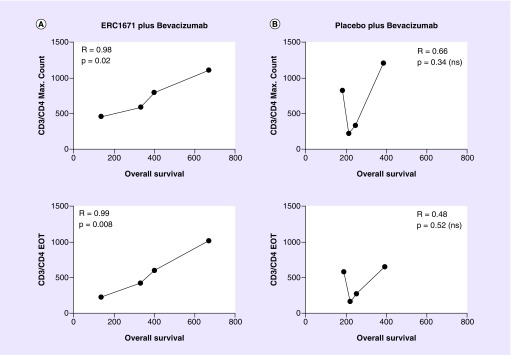
Methods: In this double-blinded, randomized, Phase II study bevacizumab-naive patients with recurrent GBM were randomized to receive either ERC1671 in combination with granulocyte-macrophage colony-stimulating factor (GM-CSF) (Leukine® or sargramostim) and cyclophosphamide plus bevacizumab, or placebo plus bevacizumab. Interim results: Median overall survival (OS) of patients treated with ERC1671 plus bevacizumab was 12 months. In the placebo plus bevacizumab group, median OS was 7.5 months. The maximal CD4+ T-lymphocyte count correlated with OS in the ERC1671 but not in the placebo group.
Conclusion: The addition of ERC1671/GM-CSF/cyclophosphamide to bevacizumab resulted in a clinically meaningful survival benefit with minimal additional toxicity.
Keywords: CD4+ T lymphocyte; ERC1671; GBM; GBM vaccine; allogeneic; autologous; bevacizumab; glioma surgery; immunotherapy.
Conflict of interest statement
This study was supported by funding from Epithopoietic Research Corporation. The study is an investigator-initiated study (DA Bota) funded by Epitopoietic Research Corporation (ERC). DA Bota has designed the study in collaboration with the study sponsor and the other investigators and managed the clinical trial database, and performed statistical analysis (with R Zidovetzki support). The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. The following authors are on the ERC advisory board, board of directors, employed by ERC or own ERC shares: TC Chen, C Pretto, V EJC Schijns and A Stathopoulos. Grant number: UCI Cancer Center Award [P30CA062203] from the National Cancer Institute. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- CBTRUS. Primary Brain and Central Nervous System Tumors Diagnosed in the United States in 2004–2007. Central Brain Tumor Registry of the United States; IL, US: 2011.
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005;352:987–996. - PubMed
-
- Stupp R, Hegi ME, Mason WP, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised Phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
-
- Stupp R, Taillibert S, Kanner AA, et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: a randomized clinical trial. JAMA. 2015;314:2535–2543. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials