

Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial
- PMID: 30158069
- PMCID: PMC7255888
- DOI: 10.1016/S0140-6736(18)31924-X
Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial
Abstract
Background: The use of aspirin in the primary prevention of cardiovascular events remains controversial. We aimed to assess the efficacy and safety of aspirin versus placebo in patients with a moderate estimated risk of a first cardiovascular event.
Methods: ARRIVE is a randomised, double-blind, placebo-controlled, multicentre study done in seven countries. Eligible patients were aged 55 years (men) or 60 years (women) and older and had an average cardiovascular risk, deemed to be moderate on the basis of the number of specific risk factors. We excluded patients at high risk of gastrointestinal bleeding or other bleeding, or diabetes. Patients were randomly assigned (1:1) with a computer-generated randomisation code to receive enteric-coated aspirin tablets (100 mg) or placebo tablets, once daily. Patients, investigators, and others involved in treatment or data analysis were masked to treatment allocation. The primary efficacy endpoint was a composite outcome of time to first occurrence of cardiovascular death, myocardial infarction, unstable angina, stroke, or transient ischaemic attack. Safety endpoints were haemorrhagic events and incidence of other adverse events, and were analysed in the intention-to-treat population. This study is registered with ClinicalTrials.gov, number NCT00501059.
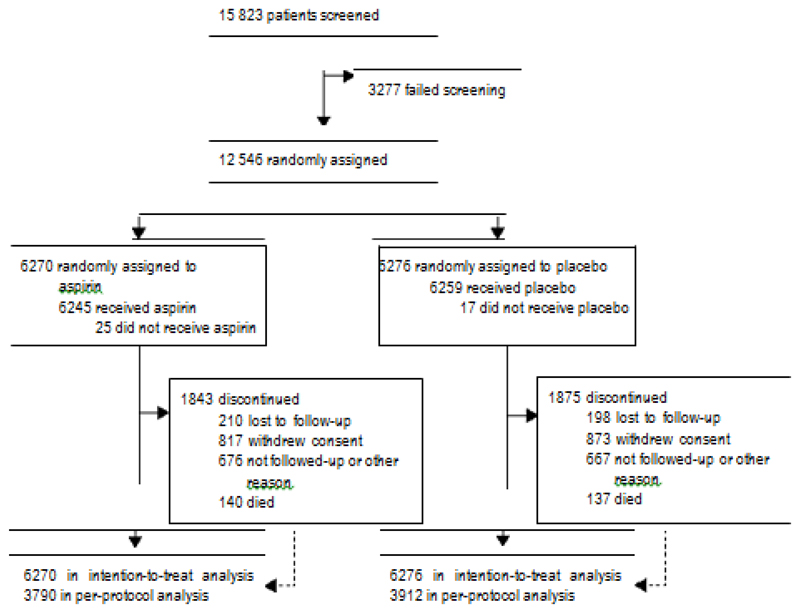
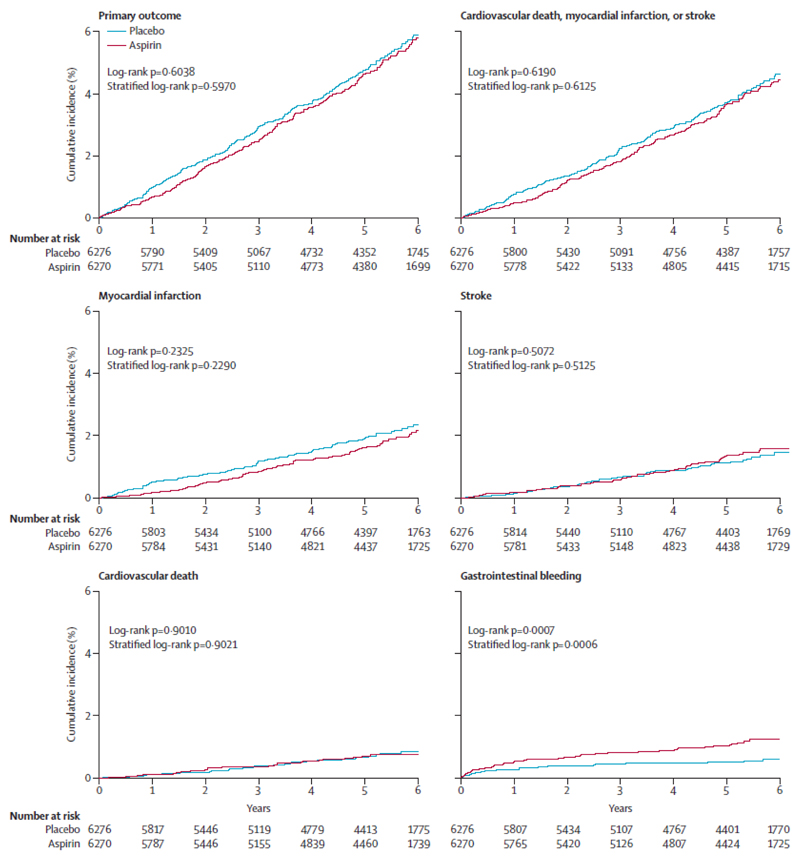
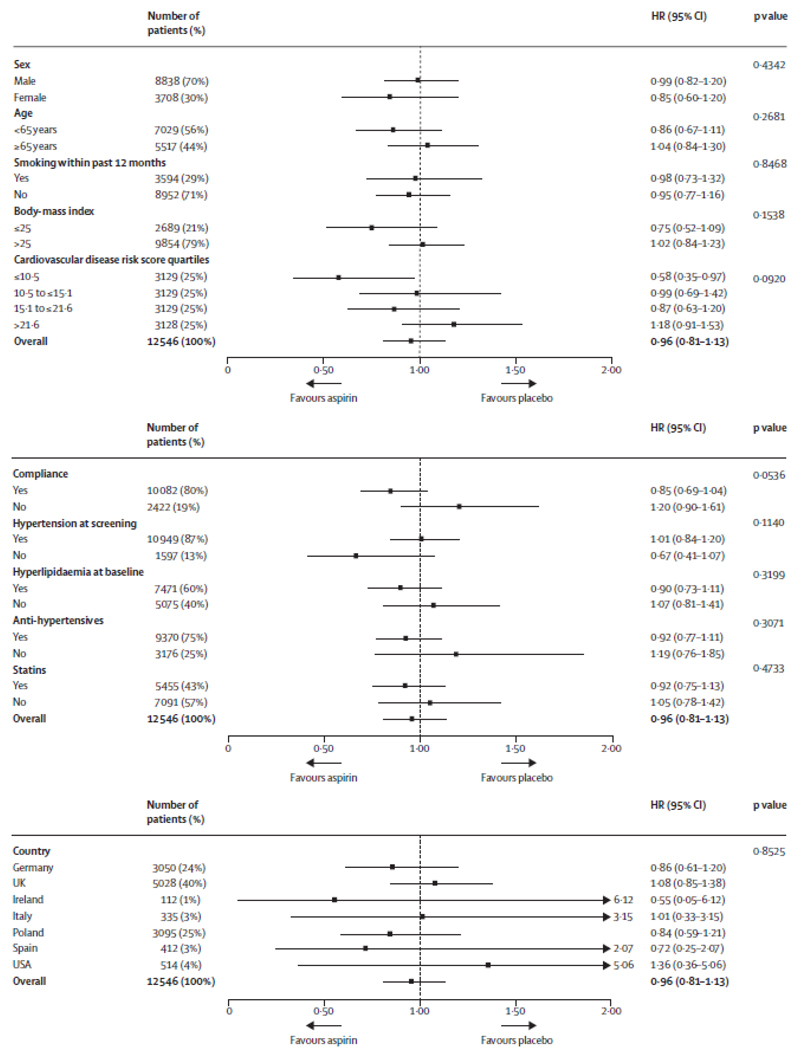
Findings: Between July 5, 2007, and Nov 15, 2016, 12 546 patients were enrolled and randomly assigned to receive aspirin (n=6270) or placebo (n=6276) at 501 study sites. Median follow-up was 60 months. In the intention-to-treat analysis, the primary endpoint occurred in 269 (4·29%) patients in the aspirin group versus 281 (4·48%) patients in the placebo group (hazard ratio [HR] 0·96; 95% CI 0·81-1·13; p=0·6038). Gastrointestinal bleeding events (mostly mild) occurred in 61 (0·97%) patients in the aspirin group versus 29 (0·46%) in the placebo group (HR 2·11; 95% CI 1·36-3·28; p=0·0007). The overall incidence rate of serious adverse events was similar in both treatment groups (n=1266 [20·19%] in the aspirin group vs n=1311 [20·89%] in the placebo group. The overall incidence of adverse events was similar in both treatment groups (n=5142 [82·01%] vs n=5129 [81·72%] in the placebo group). The overall incidence of treatment-related adverse events was low (n=1050 [16·75%] vs n=850 [13·54%] in the placebo group; p<0·0001). There were 321 documented deaths in the intention-to-treat population (n=160 [2·55%] vs n=161 [2·57%] of 6276 patients in the placebo group).
Interpretation: The event rate was much lower than expected, which is probably reflective of contemporary risk management strategies, making the study more representative of a low-risk population. The role of aspirin in primary prevention among patients at moderate risk could therefore not be addressed. Nonetheless, the findings with respect to aspirin's effects are consistent with those observed in the previously published low-risk primary prevention studies.
Funding: Bayer.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
All voting members of the ARRIVE Executive Committee (JMG, CB, CC, HD, PBG, GH, TAP, PMR, LMR, MT, and GT) received personal fees from Bayer during the conduct of the study. RC is an employee of Bayer and was a non-voting member of the Executive Committee. PMR reports personal fees from Bristol-Myers Squibb. LMR reports personal fees from Novartis, Sanofi, Medtronic, Daiichi-Sankyo, and grant funding from AstraZeneca. MT reports personal fees from Celyad, Janssen Cilag, Kowa, Perfuse Group, and Servier, outside the submitted work.
Figures
Comment in
-
Aspirin for primary prevention of cardiovascular disease.Lancet. 2018 Sep 22;392(10152):988-990. doi: 10.1016/S0140-6736(18)31990-1. Epub 2018 Aug 26. Lancet. 2018. PMID: 30158070 No abstract available.
-
[Importance of acetylsalicylic acid in primary prevention : ASCEND, ARRIVE and ASPREE as well as a meta-analysis by Rothwell et al.].Internist (Berl). 2019 Feb;60(2):209-216. doi: 10.1007/s00108-018-0541-z. Internist (Berl). 2019. PMID: 30645666 German. No abstract available.
References
-
- Guirguis-Blake JM, Evans CV, Senger CA, O’Connor EA, Whitlock EP. Aspirin for the primary prevention of cardiovascular events: a systematic evidence review for the U.S. Preventive Services Task Force. Ann Intern Med. 2016;164:804–13. - PubMed
-
- Smith SC, Jr, Benjamin EJ, Bonow RO, et al. World Heart Federation and the Preventive Cardiovascular Nurses Association. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124:2458–73. - PubMed
-
- Bibbins-Domingo K. Aspirin use for the primary prevention of cardiovascular disease and colorectal cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2016;164:836–45. - PubMed
-
- Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Eur Heart J. 2016;37:2315–81. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
