

Stimulation of the Beta2 Adrenergic Receptor at Reperfusion Limits Myocardial Reperfusion Injury via an Interleukin-10-Dependent Anti-Inflammatory Pathway in the Spleen
- PMID: 30158399
- PMCID: PMC6380896
- DOI: 10.1253/circj.CJ-18-0061
Stimulation of the Beta2 Adrenergic Receptor at Reperfusion Limits Myocardial Reperfusion Injury via an Interleukin-10-Dependent Anti-Inflammatory Pathway in the Spleen
Abstract
Background: In addition to the airway-relaxing effects, β2 adrenergic receptor (β2AR) agonists are also found to have broad anti-inflammatory effects. The current study was conducted to define the role of β2AR agonists in limiting myocardial ischemia/reperfusion injury (IRI).
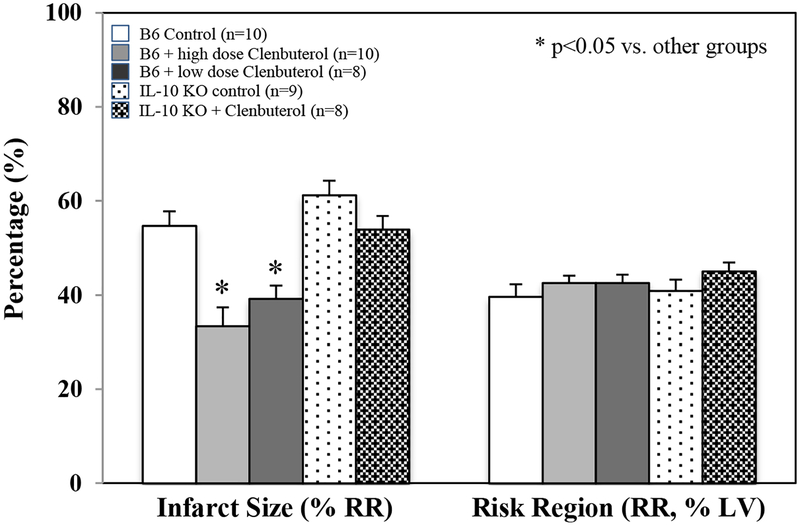
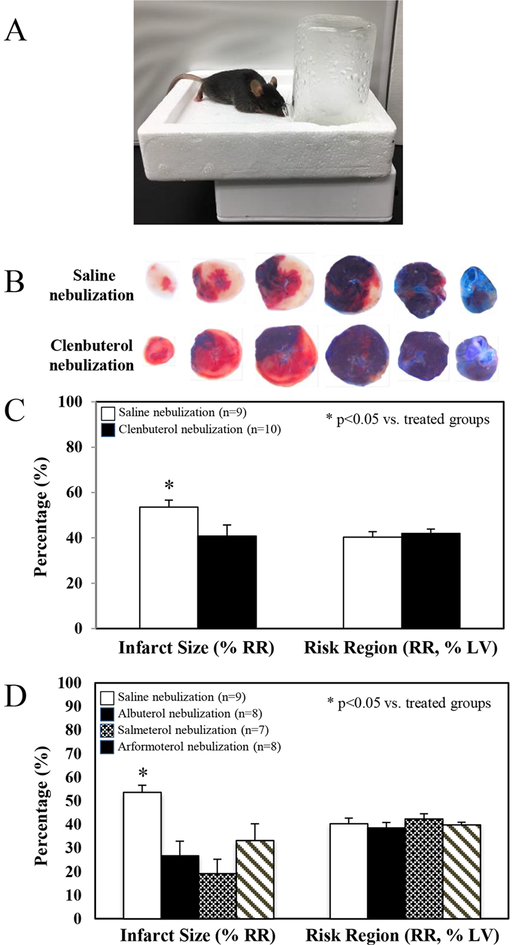
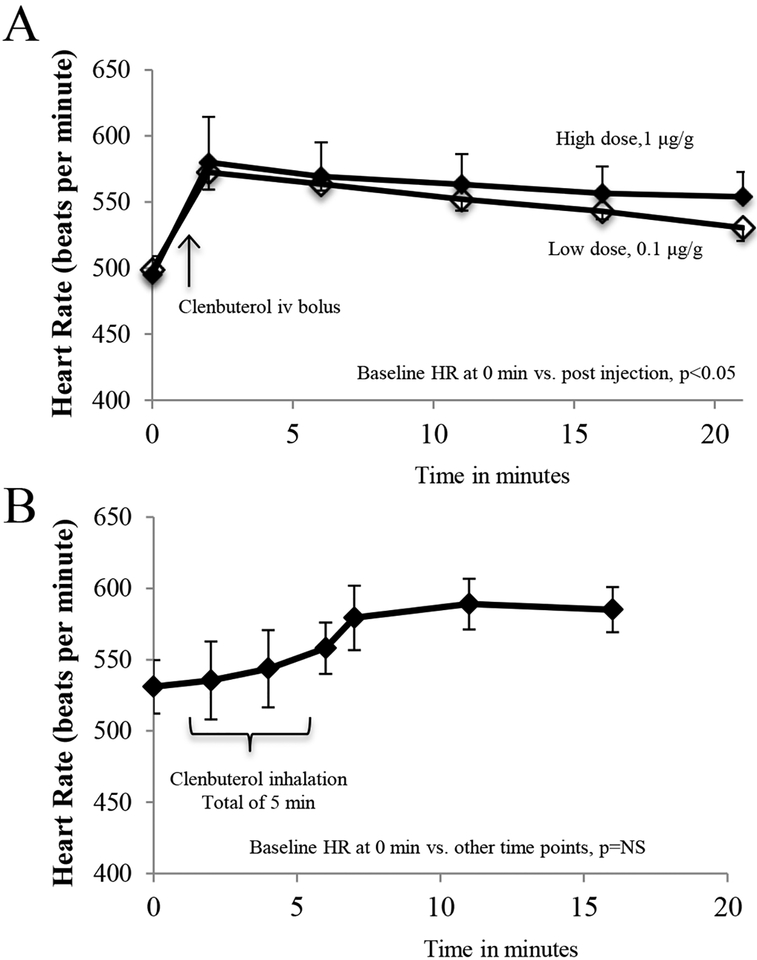
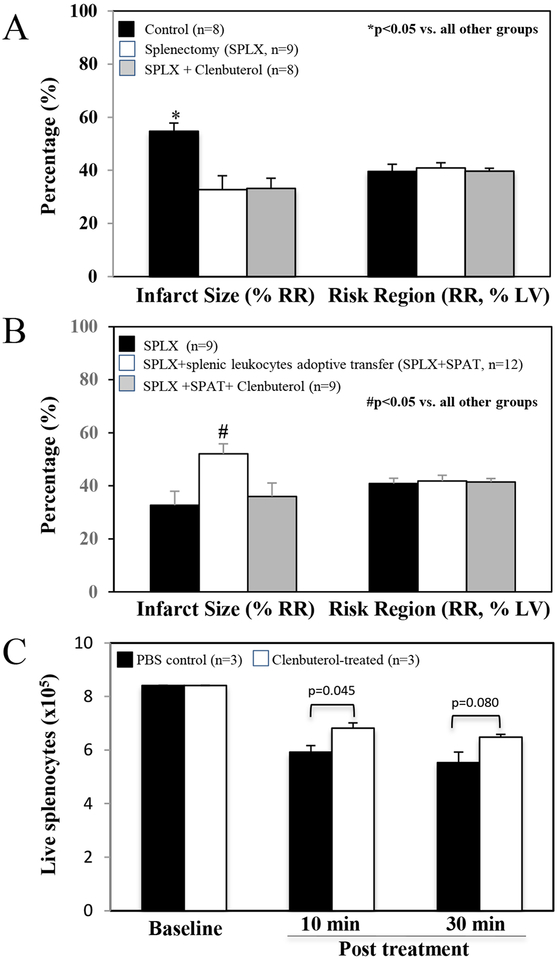
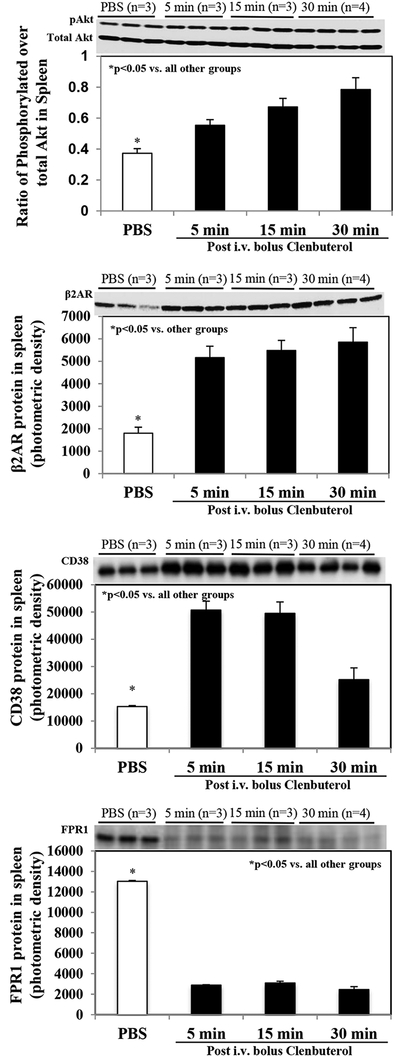
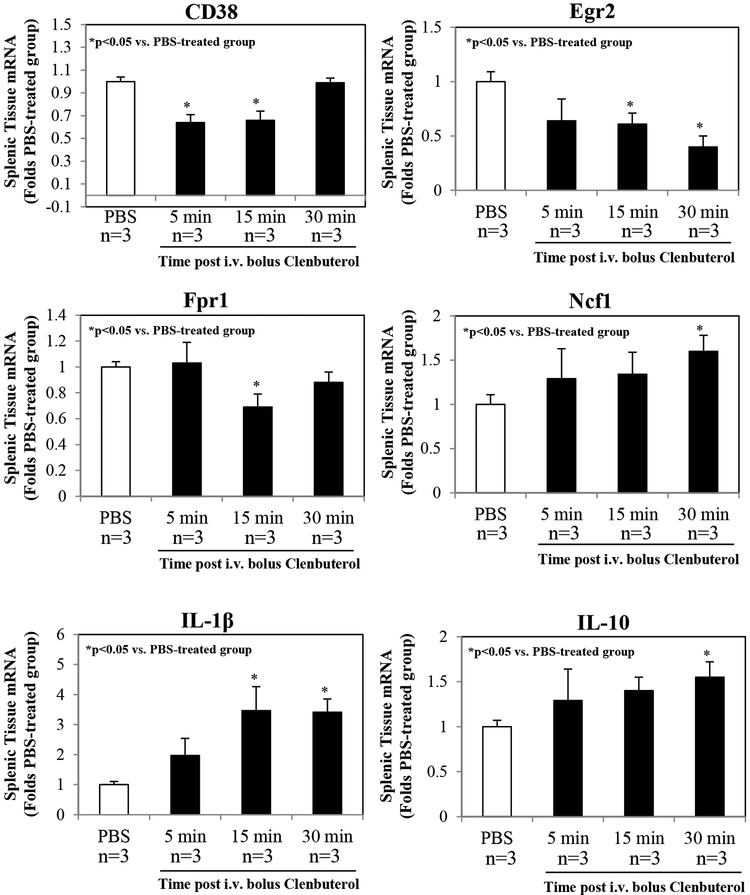
Methods and results: Adult male wild-type (WT) and interleukin (IL)-10 knockout (KO) mice underwent a 40-min left coronary artery ligation and 60-min reperfusion. A selective β2AR agonist, Clenbuterol, at doses of 0.1 μg or 1 μg/g weight i.v. 5 min before reperfusion, significantly reduced myocardial infarct size (IS) by 28% and 39% (vs. control, P<0.05) in WT mice respectively, but had no protective effect in IL-10 KO mice. Inhalational therapy with nebulized Clenbuterol, Albuterol, Salmeterol or Arformoterol immediately before ischemia significantly reduced IS (P<0.05) in WT mice. Splenectomy similarly reduced IS as Clenbuterol-treated mice, but intravenous Clenbuterol did not further reduce IS in splenectomized mice. In splenectomized WT mice, acute transfer of isolated splenocytes, not the Clenbuterol-pretreated splenocytes, restored the myocardial IS to the level of intact mice. Intravenous Clenbuterol significantly increased splenic protein levels of β2AR, phosphorylated Akt and IL-10 and plasma IL-10, and inhibited the expression of pro-inflammatory mRNAs.
Conclusions: Both intravenous and inhalational β2AR agonists exert a cardioprotective effect against IRI by activating the anti-inflammatory β2AR-IL-10 pathway.
Keywords: Clenbuterol; Heart; Ischemia/reperfusion; Myocardial infarction; β2AR.
Conflict of interest statement
Figures

References
-
- Semkova I, Schilling M, Henrich-Noack P, Rami A, Krieglstein J. Clenbuterol protects mouse cerebral cortex and rat hippocampus from ischemic damage and attenuates glutamate neurotoxicity in cultured hippocampal neurons by induction of NGF. Brain Res 1996;717:44–54. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials