

In vivo phosphoproteomics reveals kinase activity profiles that predict treatment outcome in triple-negative breast cancer
- PMID: 30158526
- PMCID: PMC6115463
- DOI: 10.1038/s41467-018-05742-z
In vivo phosphoproteomics reveals kinase activity profiles that predict treatment outcome in triple-negative breast cancer
Abstract
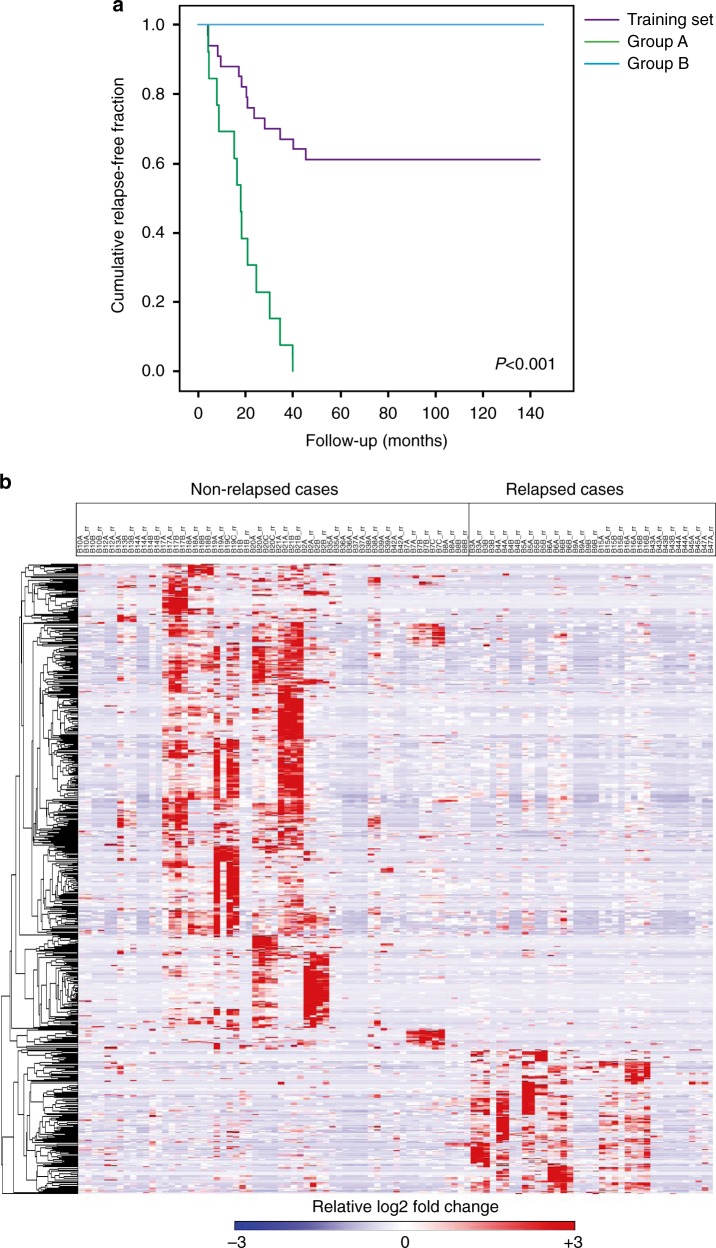
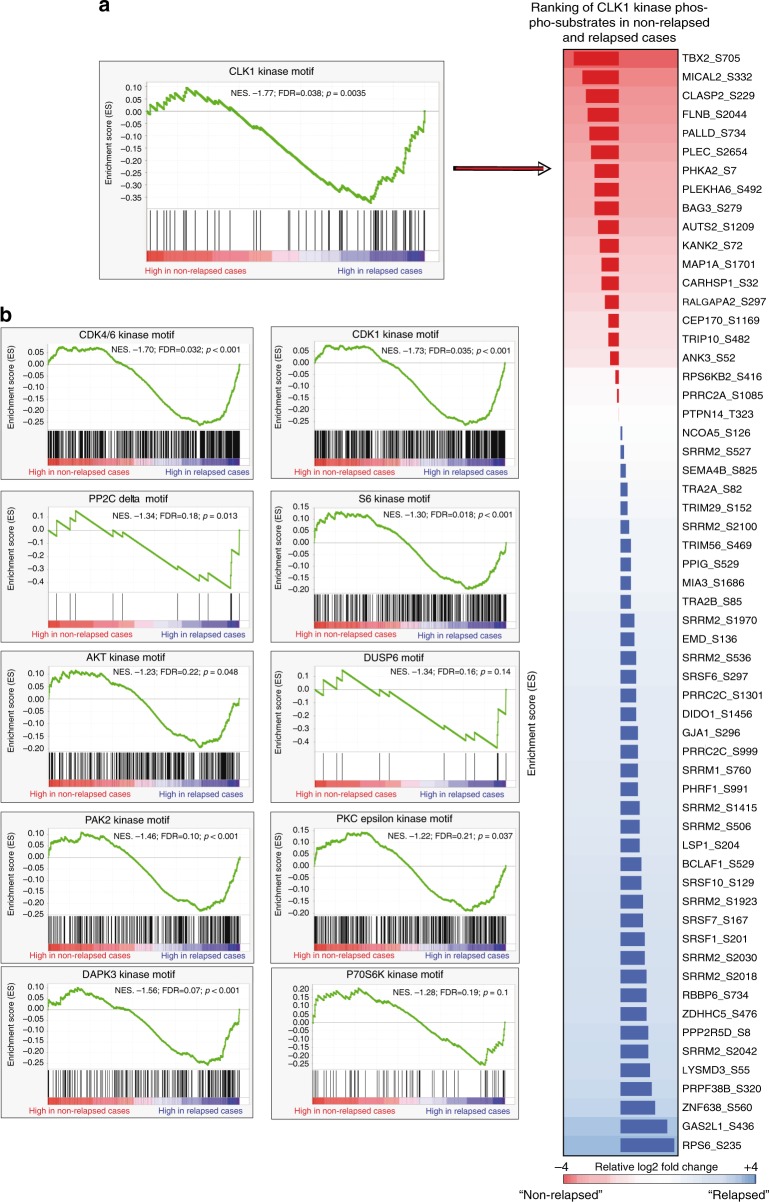
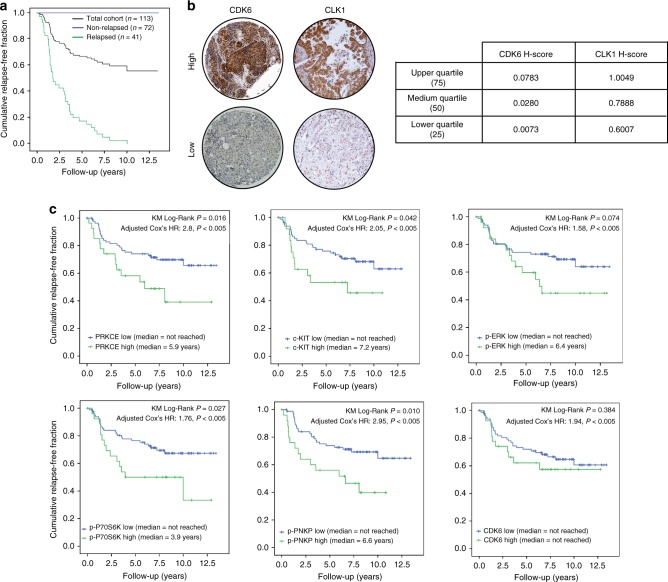
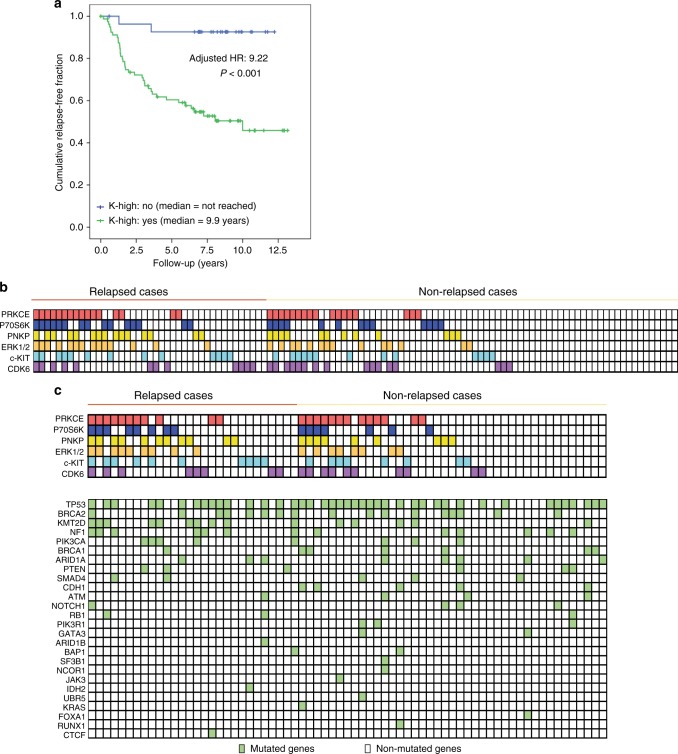
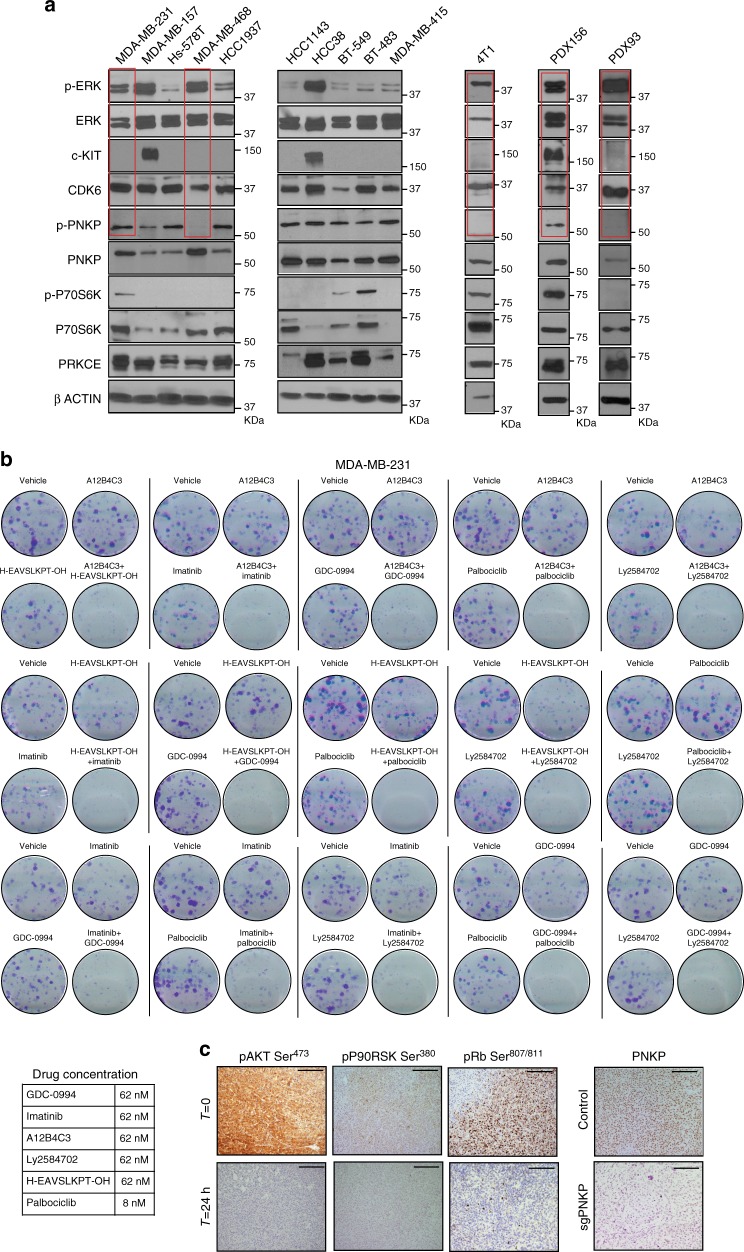
Triple-negative breast cancer (TNBC) lacks prognostic and predictive markers. Here, we use high-throughput phosphoproteomics to build a functional TNBC taxonomy. A cluster of 159 phosphosites is upregulated in relapsed cases of a training set (n = 34 patients), with 11 hyperactive kinases accounting for this phosphoprofile. A mass-spectrometry-to-immunohistochemistry translation step, assessing 2 independent validation sets, reveals 6 kinases with preserved independent prognostic value. The kinases split the validation set into two patterns: one without hyperactive kinases being associated with a >90% relapse-free rate, and the other one showing ≥1 hyperactive kinase and being associated with an up to 9.5-fold higher relapse risk. Each kinase pattern encompasses different mutational patterns, simplifying mutation-based taxonomy. Drug regimens designed based on these 6 kinases show promising antitumour activity in TNBC cell lines and patient-derived xenografts. In summary, the present study elucidates phosphosites and kinases implicated in TNBC and suggests a target-based clinical classification system for TNBC.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
