

No Guts, No Loss: Toward the Ideal Treatment for Obesity in the Twenty-First Century
- PMID: 30158899
- PMCID: PMC6104129
- DOI: 10.3389/fendo.2018.00442
No Guts, No Loss: Toward the Ideal Treatment for Obesity in the Twenty-First Century
Abstract
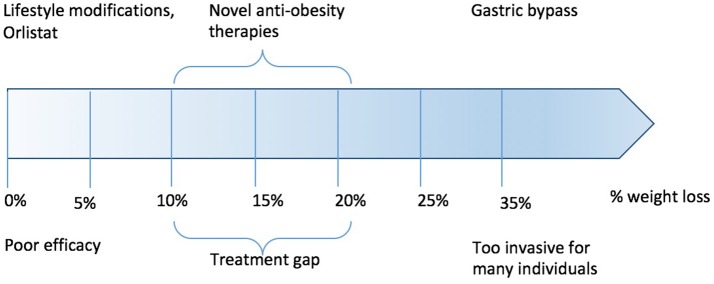
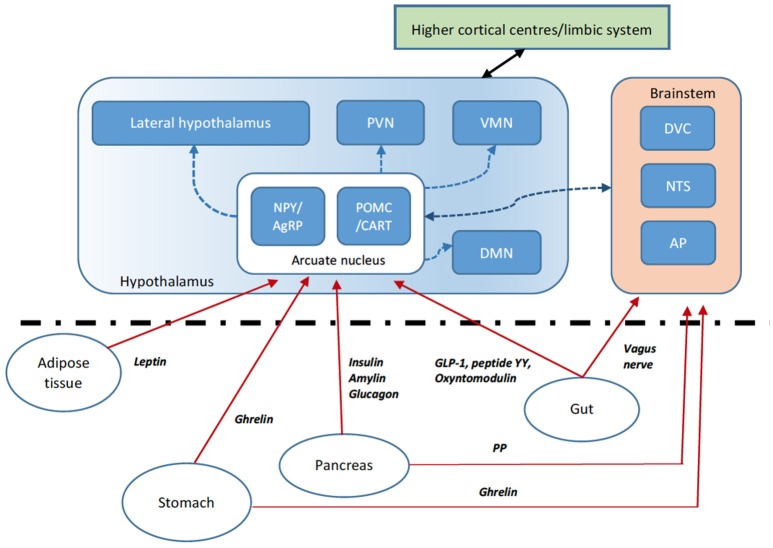
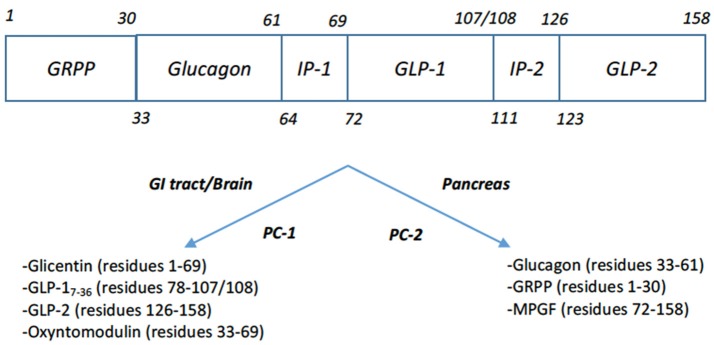
Over the last century, our knowledge of the processes which control appetite and weight regulation has developed significantly. The understanding of where gut hormones fit into the control of energy homeostasis in addition to the rapid advancement of pharmacotherapeutics has paved the way for the development of novel gut hormone analogs to target weight loss. Currently, bariatric surgery remains the most efficacious treatment for obesity. The emergence of gut hormone analogs may provide a useful non-surgical addition to the armamentarium in treating obesity. Simply targeting single gut hormone pathways may be insufficiently efficacious, and combination/multiple-agonist approaches may be necessary to obtain the results required for clear clinical impact.
Keywords: GLP-1; Oxyntomodulin; diabetes mellitus; gastric bypass surgery; glucagon; gut hormones; obesity.
Figures
References
-
- WHO Global Health Observatory Global Health Observatory Repository: Overweight/Obesity. (2018) Available online at: http://apps.who.int/gho/data/node.main.A896, 2018
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources