

Radiological Patterns of Lung Involvement in Inflammatory Bowel Disease
- PMID: 30158965
- PMCID: PMC6109524
- DOI: 10.1155/2018/5697846
Radiological Patterns of Lung Involvement in Inflammatory Bowel Disease
Abstract
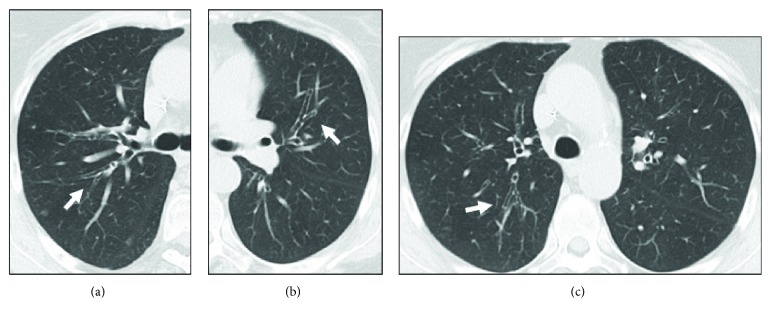
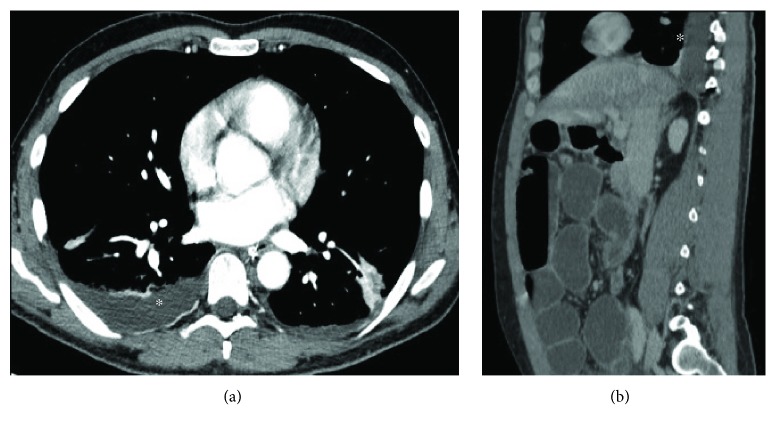
Inflammatory bowel disease (IBD) is a form of chronic inflammation of the gastrointestinal tract, including two major entities: ulcerative colitis and Crohn's disease. Although intestinal imaging of IBD is well known, imaging of extraintestinal manifestations is not extensively covered. In particular, the spectrum of IBD-associated or related changes in the chest is broad and may mimic other conditions. The common embryonic origin of intestine and lungs from the foregut, autoimmunity, smoking, and bacterial translocation from the colon may all be involved in the pathogenesis of these manifestations in IBD patients. Chest involvement in IBD can present concomitant with or years after the onset of the bowel disease even postcolectomy and can affect more than one thoracic structure. The purpose of the present paper is to present the different radiological spectrum of IBD-related chest manifestations, including lung parenchyma, airways, serosal surfaces, and pulmonary vasculature. The most prevalent and distinctive pattern of respiratory involvement is large airway inflammation, followed by lung alterations. Pulmonary manifestations are mainly detected by pulmonary function tests and high-resolution computed tomography (HRCT). It is desirable that radiologists know the various radiological patterns of possible respiratory involvement in such patients, especially at HRCT. It is essential for radiologists to work in multidisciplinary teams in order to establish the correct diagnosis and treatment, which rests on corticosteroids at variance with any other form of bronchiectasis.
Figures











References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
