

SCN1Bβ mutations that affect their association with Kv4.3 underlie early repolarization syndrome
- PMID: 30160358
- PMCID: PMC6201368
- DOI: 10.1111/jcmm.13839
SCN1Bβ mutations that affect their association with Kv4.3 underlie early repolarization syndrome
Abstract
Background: Abnormal cardiac ion channels current, including transient outward potassium current (Ito ), is associated with early repolarization syndrome (ERS). Previous studies showed that mutations in SCN1Bβ both to increase the Ito current and to decrease the sodium current. Yet its role in ERS remains unknown.
Objective: To determine the role of mutations in the SCN1Bβ subunits in ERS.
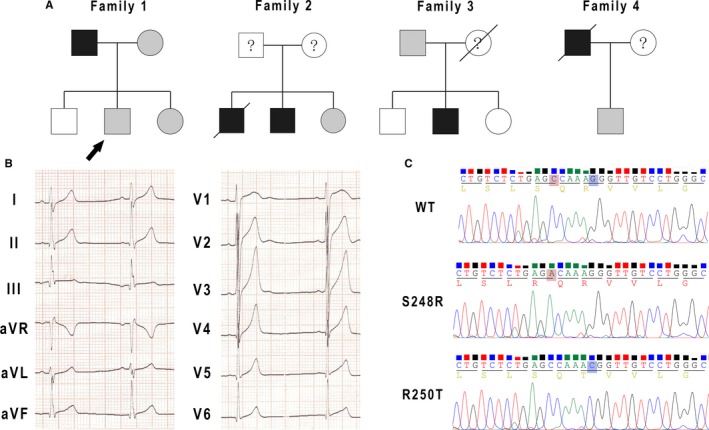
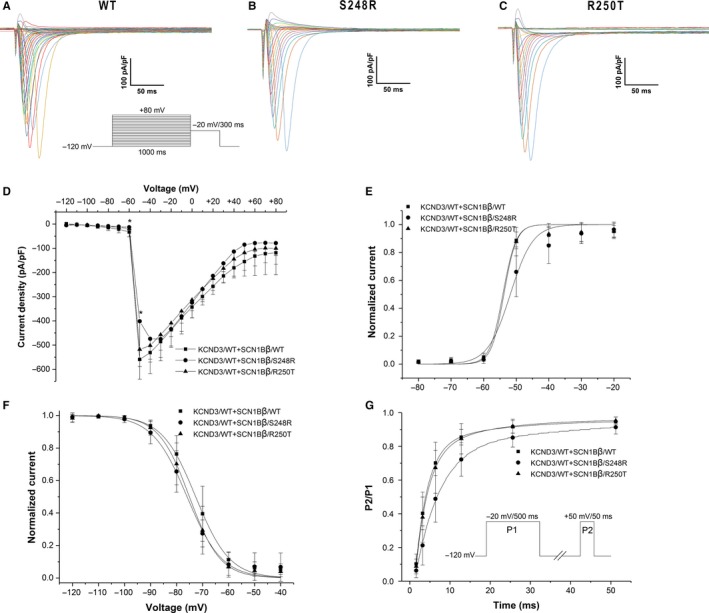
Methods: We screened for mutations in the SCN1B genes from four families with ERS. Wild-type and mutant SCN1Bβ genes were co-expressed with wild-type KCND3 in human embryonic kidney cells (HEK293). Whole-cell patch-clamp technique and co-immunoprecipitation were used to study the electrophysiological properties and explore the underlying mechanisms.
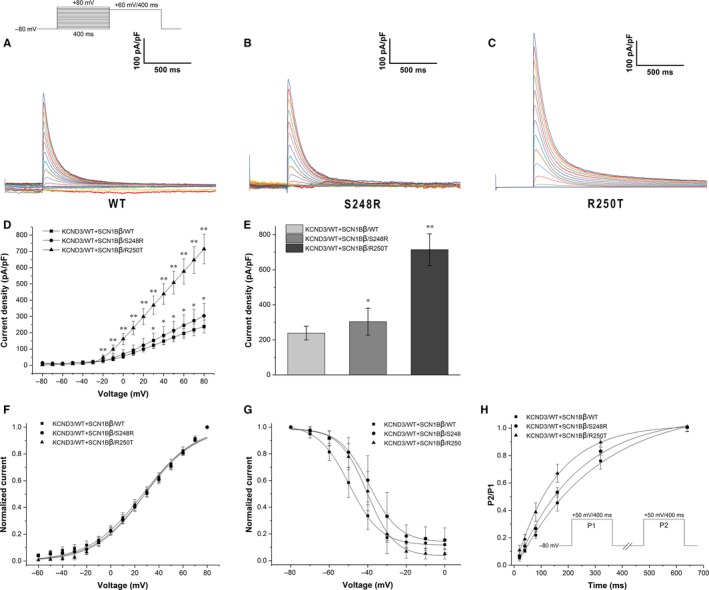
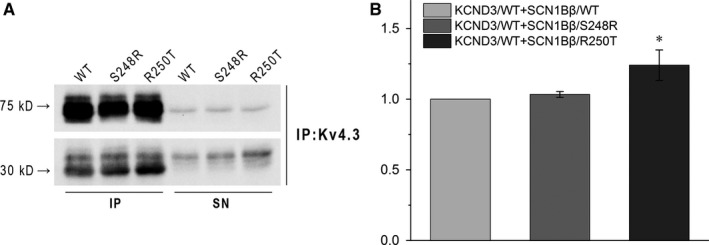
Results: S248R and R250T mutations in SCN1Bβ were detected in 4 families' probands. Neither S248R nor R250T mutation had significant influence on the sodium channel current density (INa ) when co-expressed with SCN5A/WT. Co-expression of KCND3/WT and SCN1Bβ/S248R or SCN1Bβ/R250T increased the transient outward potassium current Ito by 27.44% and 199.89%, respectively (P < 0.05 and P < 0.01, respectively) when compared with SCN1Bβ/WT. Electrophysiological properties showed that S248R and R250T mutations decreased the steady-state inactivation and recovery from inactivation of Ito channel. Co-immunoprecipitation study demonstrated an increased association between SCN1Bβ mutations and Kv4.3 compared with SCN1Bβ/WT (P < 0.05 and P < 0.01, respectively).
Conclusion: The S248R and R250T mutations of SCN1Bβ gene caused gain-of-function of Ito by associated with Kv4.3, which maybe underlie the ERS phenotype of the probands.
Keywords: SCN1Bβ; early repolarization syndrome; transient outward potassium current.
© 2018 The Authors. Journal of Cellular and Molecular Medicine published by John Wiley & Sons Ltd and Foundation for Cellular and Molecular Medicine.
Figures
Similar articles
-
Association of Cardiac Electrical Disorders With KCND3 Gene Mutation.Cureus. 2023 Feb 3;15(2):e34597. doi: 10.7759/cureus.34597. eCollection 2023 Feb. Cureus. 2023. PMID: 36883079 Free PMC article. Review.
-
A de novo gain-of-function KCND3 mutation in early repolarization syndrome.Heart Rhythm. 2019 Nov;16(11):1698-1706. doi: 10.1016/j.hrthm.2019.05.033. Epub 2019 Jun 4. Heart Rhythm. 2019. PMID: 31173922
-
Two novel Brugada syndrome-associated mutations increase KV4.3 membrane expression and function.Int J Mol Med. 2015 Jul;36(1):309-15. doi: 10.3892/ijmm.2015.2223. Epub 2015 May 26. Int J Mol Med. 2015. PMID: 26016905 Free PMC article.
-
Acacetin, a Potent Transient Outward Current Blocker, May Be a Novel Therapeutic for KCND3-Encoded Kv4.3 Gain-of-Function-Associated J-Wave Syndromes.Circ Genom Precis Med. 2022 Oct;15(5):e003238. doi: 10.1161/CIRCGEN.120.003238. Epub 2022 Jul 12. Circ Genom Precis Med. 2022. PMID: 35861988 Free PMC article.
-
KCND3-Related Neurological Disorders: From Old to Emerging Clinical Phenotypes.Int J Mol Sci. 2020 Aug 13;21(16):5802. doi: 10.3390/ijms21165802. Int J Mol Sci. 2020. PMID: 32823520 Free PMC article. Review.
Cited by
-
Primary Electrical Heart Disease-Principles of Pathophysiology and Genetics.Int J Mol Sci. 2024 Feb 2;25(3):1826. doi: 10.3390/ijms25031826. Int J Mol Sci. 2024. PMID: 38339103 Free PMC article. Review.
-
Molecular Pathways and Animal Models of Arrhythmias.Adv Exp Med Biol. 2024;1441:1057-1090. doi: 10.1007/978-3-031-44087-8_67. Adv Exp Med Biol. 2024. PMID: 38884769
-
Association of Cardiac Electrical Disorders With KCND3 Gene Mutation.Cureus. 2023 Feb 3;15(2):e34597. doi: 10.7759/cureus.34597. eCollection 2023 Feb. Cureus. 2023. PMID: 36883079 Free PMC article. Review.
-
Abnormal Scn1b and Fxyd1 gene expression in the pulled-through ganglionic colon may influence functional outcome in patients with Hirschsprung's disease.Pediatr Surg Int. 2019 Jan;35(1):9-14. doi: 10.1007/s00383-018-4370-x. Epub 2018 Nov 1. Pediatr Surg Int. 2019. PMID: 30386899
-
KCND3 potassium channel gene variant confers susceptibility to electrocardiographic early repolarization pattern.JCI Insight. 2019 Dec 5;4(23):e131156. doi: 10.1172/jci.insight.131156. JCI Insight. 2019. PMID: 31600170 Free PMC article.
References
-
- Steinfurt J, Odening KE. Early repolarization: a risk factor in Brugada syndrome. J Am Coll Cardiol. 2015;66(2):205‐206. - PubMed
-
- Mahida S, Derval N, Sacher F, et al. Role of electrophysiological studies in predicting risk of ventricular arrhythmia in early repolarization syndrome. J Am Coll Cardiol. 2015;65(2):151‐159. - PubMed
-
- Wu SH, Lin XX, Cheng YJ, Qiang CC, Zhang J. Early repolarization pattern and risk for arrhythmia death: a meta‐analysis. J Am Coll Cardiol. 2013;61(6):645‐650. - PubMed
-
- Junttila MJ, Sager SJ, Tikkanen JT, Anttonen O, Huikuri HV, Myerburg RJ. Clinical significance of variants of J‐points and J‐waves: early repolarization patterns and risk. Eur Heart J. 2012;33(21):2639‐2643. - PubMed
-
- Tikkanen JT, Junttila MJ, Anttonen O, et al. Early repolarization: electrocardiographic phenotypes associated with favorable long‐term outcome. Circulation. 2011;123(23):2666‐2673. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
