

The impact of geographic access on institutional delivery care use in low and middle-income countries: Systematic review and meta-analysis
- PMID: 30161201
- PMCID: PMC6117044
- DOI: 10.1371/journal.pone.0203130
The impact of geographic access on institutional delivery care use in low and middle-income countries: Systematic review and meta-analysis
Abstract
Background: Geographic access to obstetric care facilities has a significant influence on women's uptake of institutional delivery care. However, this effect was not consistent across studies. Some studies reported that geographic access to obstetric care facilities had no influence on the use of facility delivery. Therefore, this systematic review and meta-analysis synthesized and pooled the influence of geographic access on institutional delivery service uptake in low and middle-income countries.
Methods: Multiple combinations of search terms were used to search articles from six databases and a hand search of reference lists performed. We included observational studies conducted in low and middle-income countries which reported the influence of geographic access on delivery care use. The pooled effects of geographic access on institutional delivery care use were calculated using a random-effects model with a 95% confidence interval.
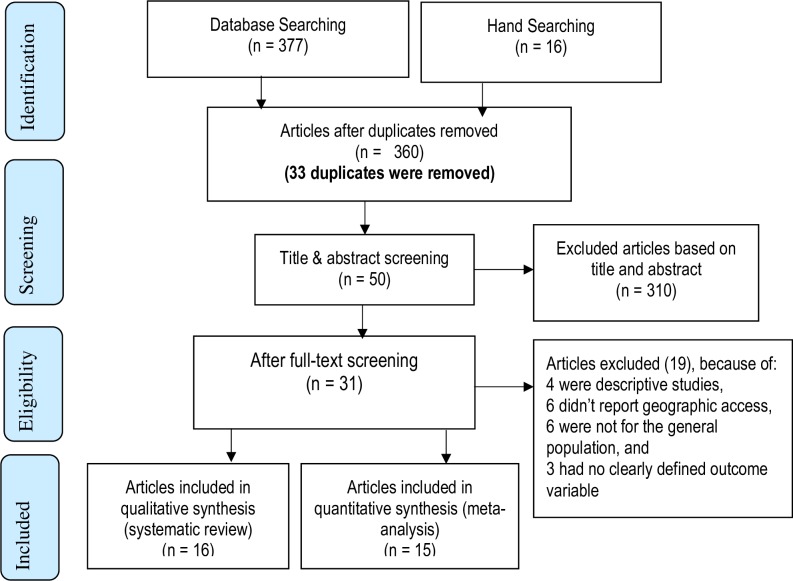
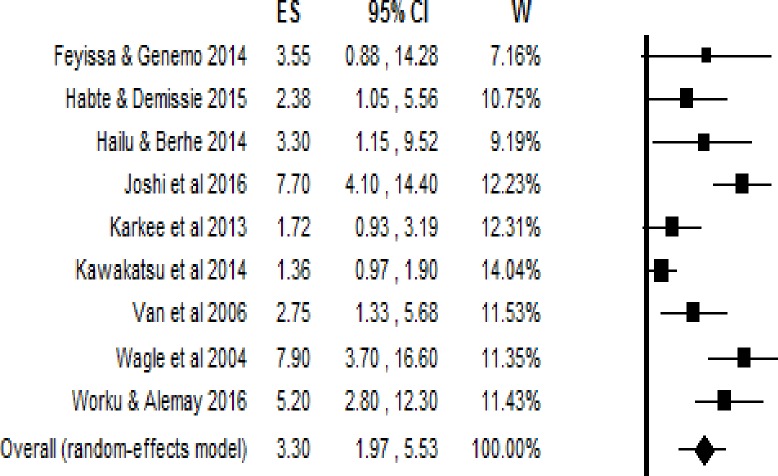
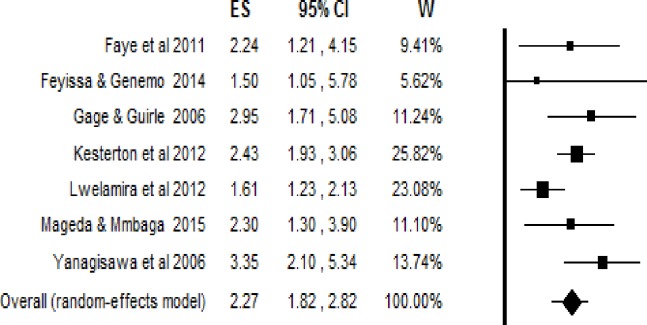
Findings: In this study a total of 31 studies were included. Among these studies, 15 met criteria for inclusion in the meta-analyses, while the remaining 16 were summarized using qualitative synthesis. Studies included in the analysis where women had to walk 60 minutes or less to access a health facility delivery were significantly heterogeneous. Having access to obstetric care facilities within five kilometres was significantly associated with institutional deliveries (pooled OR = 2.27; 95% CI = 1.82, 2.82). Similarly, a travelling time of 60 minutes or less was significantly associated with higher odds of health facility delivery (pooled OR = 3.30; 95% CI = 1.97, 5.53). Every one-hour and one-kilometre increase in travel time and distance, respectively, was negatively associated with institutional delivery care use.
Interpretation: Geographic access measured in either physical distance and/or travel time was significantly associated with women's use of facility delivery. The greater the distance and/or travel time to obstetric care facilities, the greater the barrier and the lesser the service uptake.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Primary health care: 25 years after ALMA-ATA. 2003.
-
- Gibbons L, Belizán JM, Lauer JA, Betrán AP, Merialdi M, Althabe F. The global numbers and costs of additionally needed and unnecessary caesarean sections performed per year: overuse as a barrier to universal coverage. World health report. 2010;30:1–31.
-
- Paxton A, Bailey P, Lobis S, Fry D. Global patterns in availability of emergency obstetric care. International Journal of Gynecology & Obstetrics. 2006;93(3):300–7. - PubMed
-
- Gabrysch S, Simushi V, Campbell OM. Availability and distribution of, and geographic access to emergency obstetric care in Zambia. International Journal of Gynecology & Obstetrics. 2011;114(2):174–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
