

Impact of TP53 mutation status on systemic treatment outcome in ALK-rearranged non-small-cell lung cancer
- PMID: 30165392
- PMCID: PMC6225899
- DOI: 10.1093/annonc/mdy333
Impact of TP53 mutation status on systemic treatment outcome in ALK-rearranged non-small-cell lung cancer
Abstract
Background: We analyzed whether co-occurring mutations influence the outcome of systemic therapy in ALK-rearranged non-small-cell lung cancer (NSCLC).
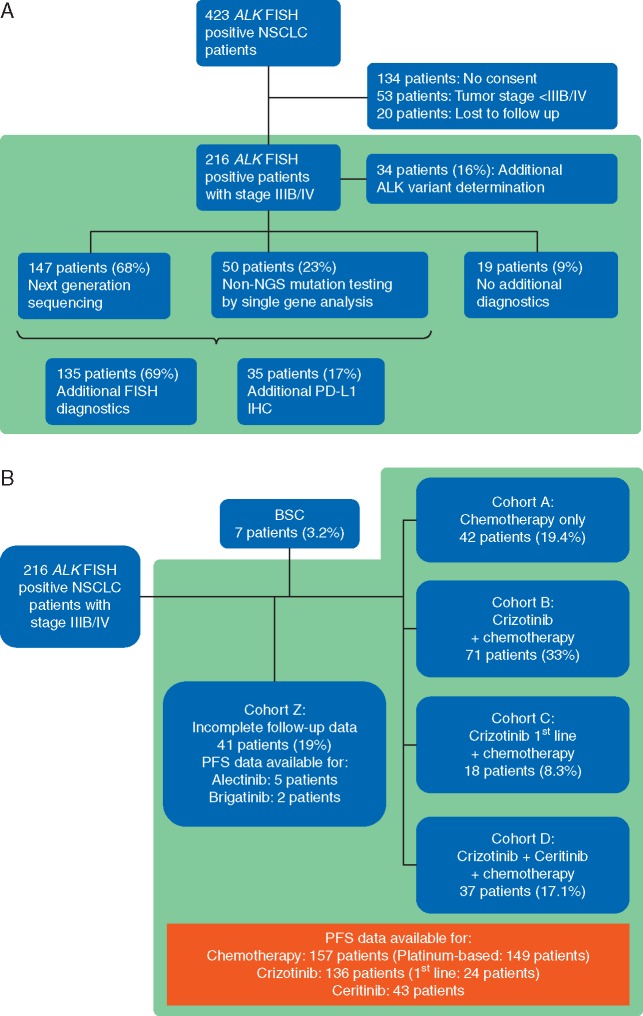
Patients and methods: ALK-rearranged stage IIIB/IV NSCLC patients were analyzed with next-generation sequencing and fluorescence in situ hybridization analyses on a centralized diagnostic platform. Median progression-free survival (PFS) and overall survival (OS) were determined in the total cohort and in treatment-related sub-cohorts. Cox regression analyses were carried out to exclude confounders.
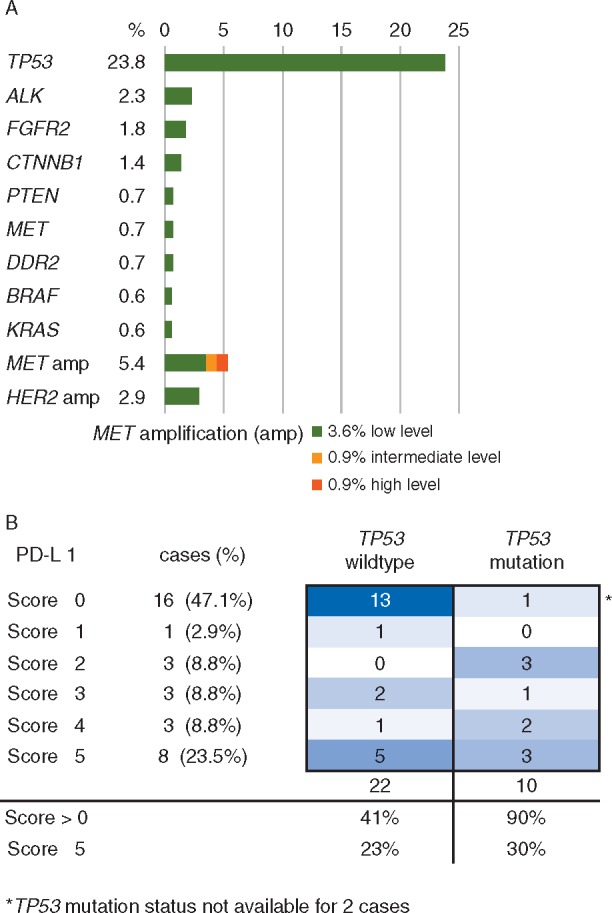
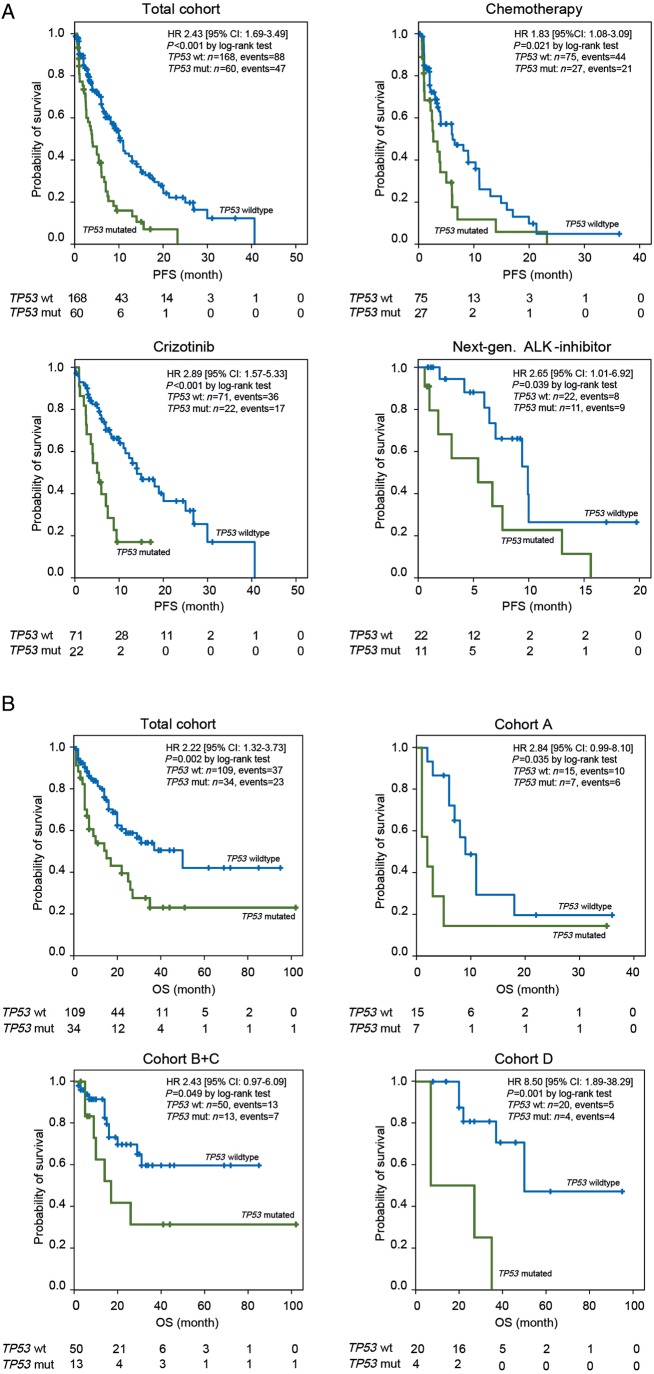
Results: Among 216 patients with ALK-rearranged NSCLC, the frequency of pathogenic TP53 mutations was 23.8%, while other co-occurring mutations were rare events. In ALK/TP53 co-mutated patients, median PFS and OS were significantly lower compared with TP53 wildtype patients [PFS 3.9 months (95% CI: 2.4-5.6) versus 10.3 months (95% CI: 8.6-12.0), P < 0.001; OS 15.0 months (95% CI: 5.0-24.9) versus 50.0 months (95% CI: 22.9-77.1), P = 0.002]. This difference was confirmed in all treatment-related subgroups including chemotherapy only [PFS first-line chemotherapy 2.6 months (95% CI: 1.3-4.1) versus 6.2 months (95% CI: 1.8-10.5), P = 0.021; OS 2.0 months (95% CI: 0.0-4.6) versus 9.0 months (95% CI: 6.1-11.9), P = 0.035], crizotinib plus chemotherapy [PFS crizotinib 5.0 months (95% CI: 2.9-7.2) versus 14.0 months (95% CI: 8.0-20.1), P < 0.001; OS 17.0 months (95% CI: 6.7-27.3) versus not reached, P = 0.049] and crizotinib followed by next-generation ALK-inhibitor [PFS next-generation inhibitor 5.4 months (95% CI: 0.1-10.7) versus 9.9 months (95% CI: 6.4-13.5), P = 0.039; OS 7.0 months versus 50.0 months (95% CI: not reached), P = 0.001).
Conclusions: In ALK-rearranged NSCLC co-occurring TP53 mutations predict an unfavorable outcome of systemic therapy. Our observations encourage future research to understand the underlying molecular mechanisms and to improve treatment outcome of the ALK/TP53 co-mutated subgroup.
Figures
Comment in
-
TP53 mutations are predictive and prognostic when co-occurring with ALK rearrangements in lung cancer.Ann Oncol. 2018 Oct 1;29(10):2028-2030. doi: 10.1093/annonc/mdy339. Ann Oncol. 2018. PMID: 30265285 Free PMC article. No abstract available.
References
-
- Inamura K, Takeuchi K, Togashi Y. et al. EML4-ALK lung cancers are characterized by rare other mutations, a TTF-1 cell lineage, an acinar histology, and young onset. Mod Pathol 2009; 22(4): 508–515. - PubMed
-
- Shaw AT, Kim D-W, Nakagawa K. et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N Engl J Med 2013; 368(25): 2385–2394. - PubMed
-
- Solomon BJ, Mok T, Kim D-W. et al. First-line crizotinib versus chemotherapy in ALK-positive lung cancer. N Engl J Med 2014; 371(23): 2167–2177. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
