

A Prognostic Model of Persistent Bacteremia and Mortality in Complicated Staphylococcus aureus Bloodstream Infection
- PMID: 30165412
- PMCID: PMC6481998
- DOI: 10.1093/cid/ciy739
A Prognostic Model of Persistent Bacteremia and Mortality in Complicated Staphylococcus aureus Bloodstream Infection
Abstract
Background: Staphylococcus aureus is a leading cause of bacteremia, yet there remains a significant knowledge gap in the identification of relevant biomarkers that predict clinical outcomes. Heterogeneity in the host response to invasive S. aureus infection suggests that specific biomarker signatures could be utilized to differentiate patients prone to severe disease, thereby facilitating earlier implementation of more aggressive therapies.
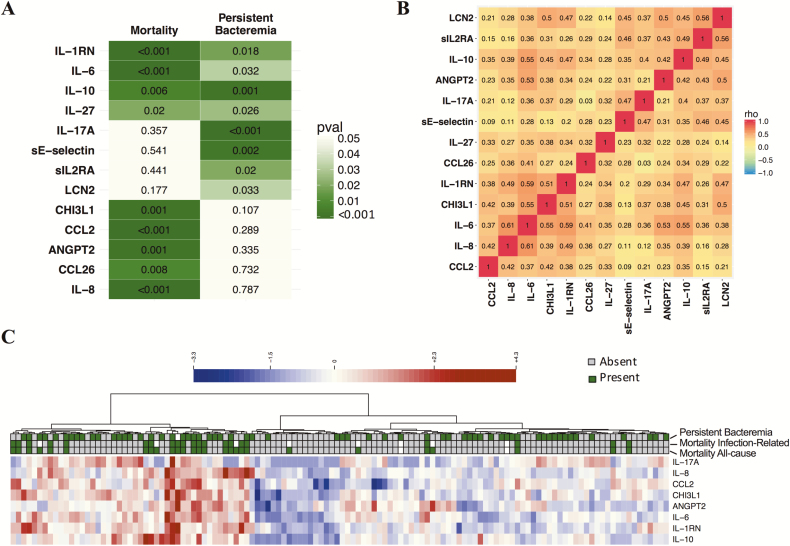
Methods: To further elucidate the inflammatory correlates of poor clinical outcomes in patients with S. aureus bacteremia, we evaluated the association between a panel of blood proteins at initial presentation of bacteremia and disease severity outcomes using 2 cohorts of patients with S. aureus bacteremia (n = 32 and n = 124).
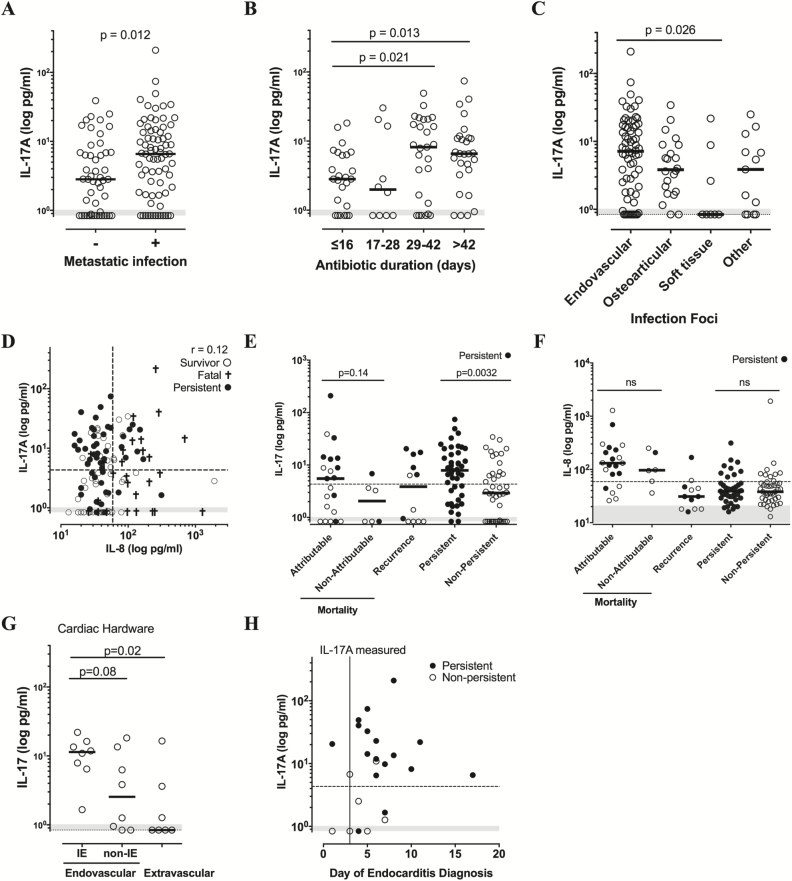
Results: We identified 13 candidate proteins that were correlated with mortality and persistent bacteremia. Prognostic modeling identified interleukin (IL)-8 and CCL2 as the strongest individual predictors of mortality, with the combination of these biomarkers classifying fatal outcome with 89% sensitivity and 77% specificity (P < .0001). Baseline IL-17A levels were elevated in patients with persistent bacteremia (P < .0001), endovascular (P = .026) and metastatic tissue infections (P = .012).
Conclusions: These results demonstrate the potential utility of selected biomarkers to distinguish patients with the highest risk for treatment failure and bacteremia-related complications, providing a valuable tool for clinicians in the management of S. aureus bacteremia. Additionally, these biomarkers could identify patients with the greatest potential to benefit from novel therapies in clinical trials.
Keywords: Staphylococcus aureus; bacteremia; endocarditis; prognostic biomarkers.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures



References
-
- Corey GR. Staphylococcus aureus bloodstream infections: definitions and treatment. Clin Infect Dis 2009; 48(Suppl 4):S254–9. - PubMed
-
- Lindsay JA, Holden MT. Understanding the rise of the superbug: investigation of the evolution and genomic variation of Staphylococcus aureus. Funct Integr Genomics 2006; 6:186–201. - PubMed
-
- Fowler VG Jr, Olsen MK, Corey GR, et al. Clinical identifiers of complicated Staphylococcus aureus bacteremia. Arch Intern Med 2003; 163:2066–72. - PubMed
-
- Casapao AM, Jacobs DM, Bowers DR, Beyda ND, Dilworth TJ; REACH-ID Study Group Early administration of adjuvant β-lactam therapy in combination with vancomycin among patients with methicillin-resistant Staphylococcus aureus bloodstream infection: a retrospective, multicenter analysis. Pharmacotherapy 2017; 37:1347–56. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
