

Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF
- PMID: 30165580
- PMCID: PMC6927847
- DOI: 10.1093/eurheartj/ehy531
Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF
Erratum in
-
Corrigendum to: Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF.Eur Heart J. 2019 Feb 7;40(6):541. doi: 10.1093/eurheartj/ehy804. Eur Heart J. 2019. PMID: 30476021 Free PMC article. No abstract available.
Abstract
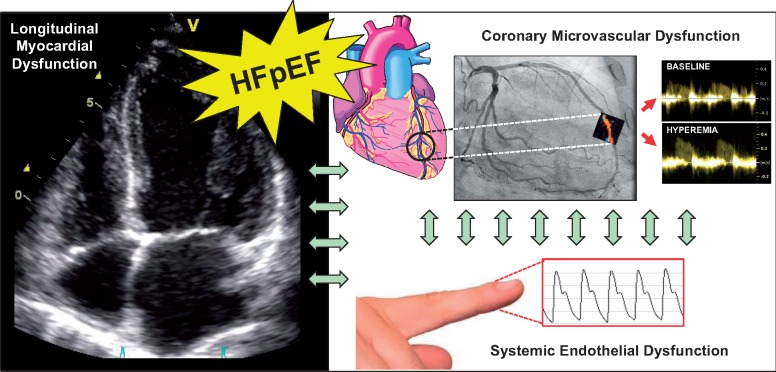
Aims: To date, clinical evidence of microvascular dysfunction in patients with heart failure (HF) with preserved ejection fraction (HFpEF) has been limited. We aimed to investigate the prevalence of coronary microvascular dysfunction (CMD) and its association with systemic endothelial dysfunction, HF severity, and myocardial dysfunction in a well defined, multi-centre HFpEF population.
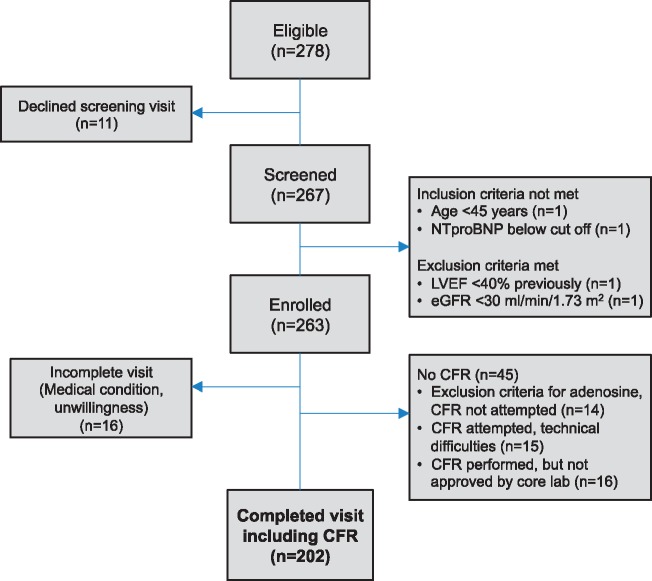
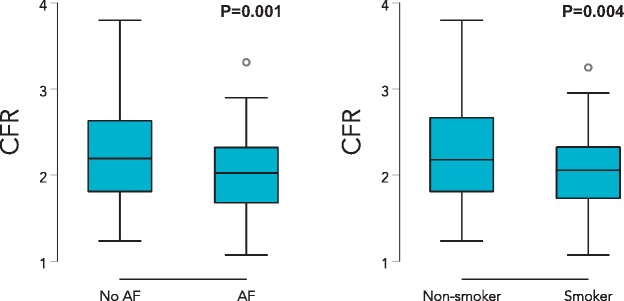
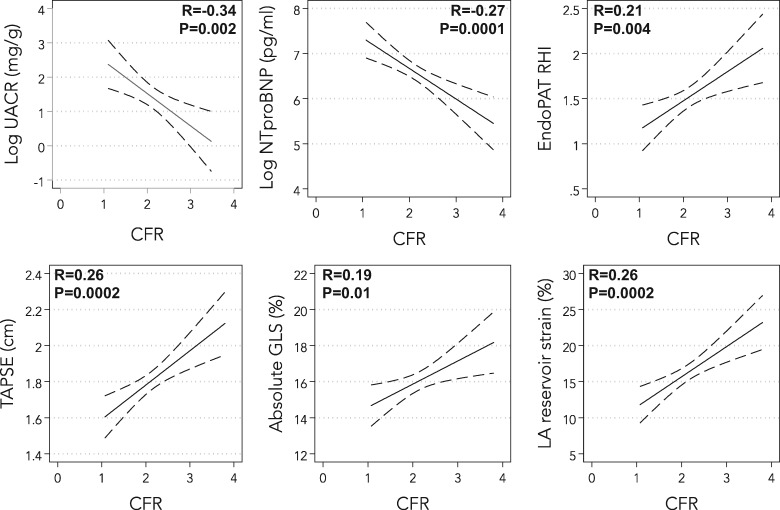
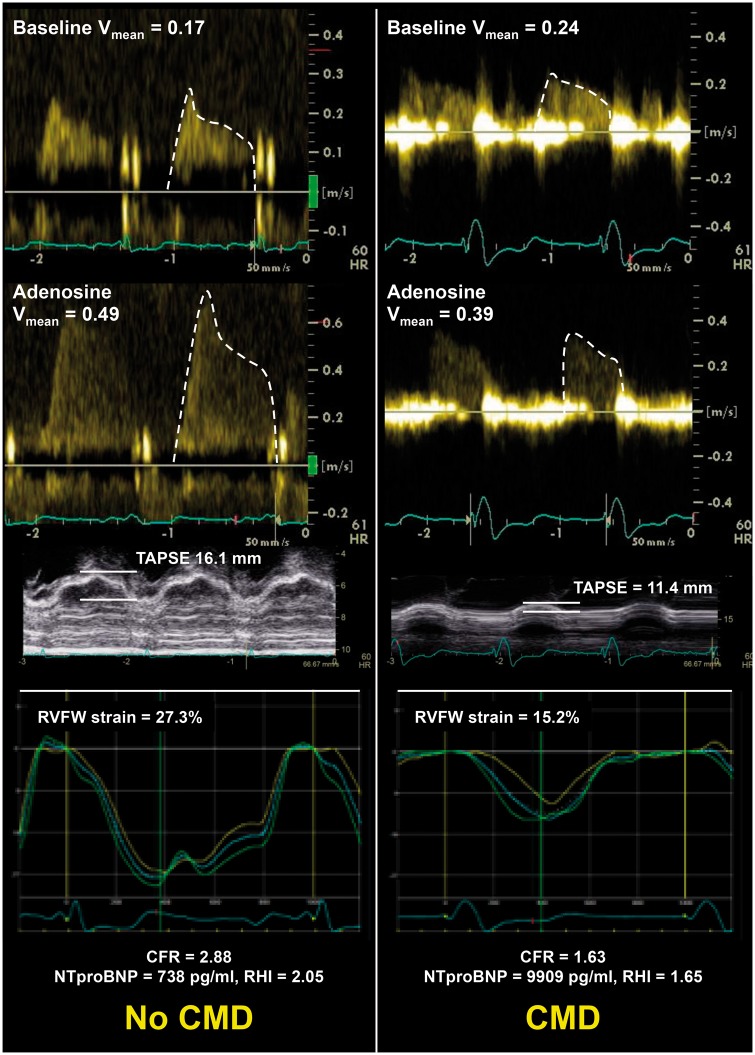
Methods and results: This prospective multinational multi-centre observational study enrolled patients fulfilling strict criteria for HFpEF according to current guidelines. Those with known unrevascularized macrovascular coronary artery disease (CAD) were excluded. Coronary flow reserve (CFR) was measured with adenosine stress transthoracic Doppler echocardiography. Systemic endothelial function [reactive hyperaemia index (RHI)] was measured by peripheral arterial tonometry. Among 202 patients with HFpEF, 151 [75% (95% confidence interval 69-81%)] had CMD (defined as CFR <2.5). Patients with CMD had a higher prevalence of current or prior smoking (70% vs. 43%; P = 0.0006) and atrial fibrillation (58% vs. 25%; P = 0.004) compared with those without CMD. Worse CFR was associated with higher urinary albumin-to-creatinine ratio (UACR) and NTproBNP, and lower RHI, tricuspid annular plane systolic excursion, and right ventricular (RV) free wall strain after adjustment for age, sex, body mass index, atrial fibrillation, diabetes, revascularized CAD, smoking, left ventricular mass, and study site (P < 0.05 for all associations).
Conclusions: PROMIS-HFpEF is the first prospective multi-centre, multinational study to demonstrate a high prevalence of CMD in HFpEF in the absence of unrevascularized macrovascular CAD, and to show its association with systemic endothelial dysfunction (RHI, UACR) as well as markers of HF severity (NTproBNP and RV dysfunction). Microvascular dysfunction may be a promising therapeutic target in HFpEF.
Figures
Comment in
-
Why do we care about coronary microvascular dysfunction and heart failure with preserved ejection fraction: addressing knowledge gaps for evidence-based guidelines.Eur Heart J. 2018 Oct 1;39(37):3451-3453. doi: 10.1093/eurheartj/ehy558. Eur Heart J. 2018. PMID: 30165471 Free PMC article. No abstract available.
-
Reply to the commentary: Prevalence and correlates of coronary microvascular dysfunction in heart failure with preserved ejection fraction: PROMIS-HFpEF.Eur Heart J. 2019 Nov 1;40(41):3434. doi: 10.1093/eurheartj/ehz473. Eur Heart J. 2019. PMID: 31292627 No abstract available.
References
-
- Franssen C, Chen S, Unger A, Korkmaz HI, De Keulenaer GW, Tschope C, Leite-Moreira AF, Musters R, Niessen HW, Linke WA, Paulus WJ, Hamdani N.. Myocardial microvascular inflammatory endothelial activation in heart failure with preserved ejection fraction. JACC Heart Fail 2016;4:312–324. - PubMed
-
- Lam CS, Brutsaert DL.. Endothelial dysfunction: a pathophysiologic factor in heart failure with preserved ejection fraction. J Am Coll Cardiol 2012;60:1787–1789. - PubMed
-
- Lam CS, Lund LH.. Microvascular endothelial dysfunction in heart failure with preserved ejection fraction. Heart 2016;102:257–259. - PubMed
-
- Paulus WJ, Tschope C.. A novel paradigm for heart failure with preserved ejection fraction: comorbidities drive myocardial dysfunction and remodeling through coronary microvascular endothelial inflammation. J Am Coll Cardiol 2013;62:263–271. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
