

Long-term Stability of Resistance to Latent Mycobacterium tuberculosis Infection in Highly Exposed Tuberculosis Household Contacts in Kampala, Uganda
- PMID: 30165605
- PMCID: PMC6495009
- DOI: 10.1093/cid/ciy751
Long-term Stability of Resistance to Latent Mycobacterium tuberculosis Infection in Highly Exposed Tuberculosis Household Contacts in Kampala, Uganda
Abstract
Background: Resistance to latent Mycobacterium tuberculosis (M.tb) infection, identified by persistently negative tuberculin skin tests (TST) and interferon-gamma release assays (IGRA), after close contact with pulmonary tuberculosis (TB) patients has not been extensively characterized. Stability of this "resistance" beyond 2 years from exposure is unknown.
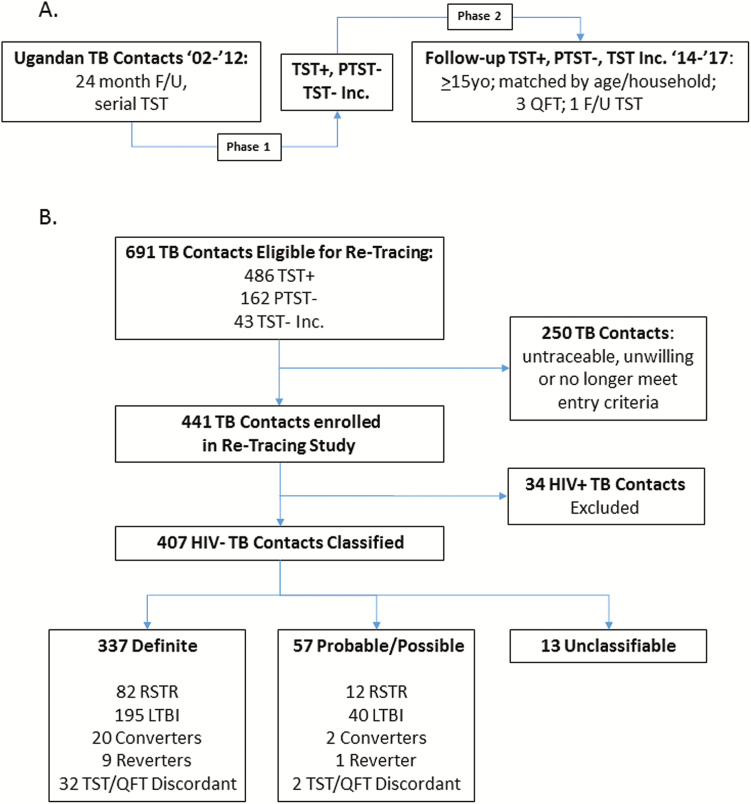
Methods: 407 of 657 eligible human immunodeficiency virus (HIV)-negative adults from a TB household contact study with persistently negative TST (PTST-) or with stable latent M.tb infection (LTBI) were retraced 9.5 years (standard deviation = 3.2) later. Asymptomatic retraced contacts underwent 3 IGRAs and follow-up TST, and their M.tb infection status classified as definite/possible/probable.
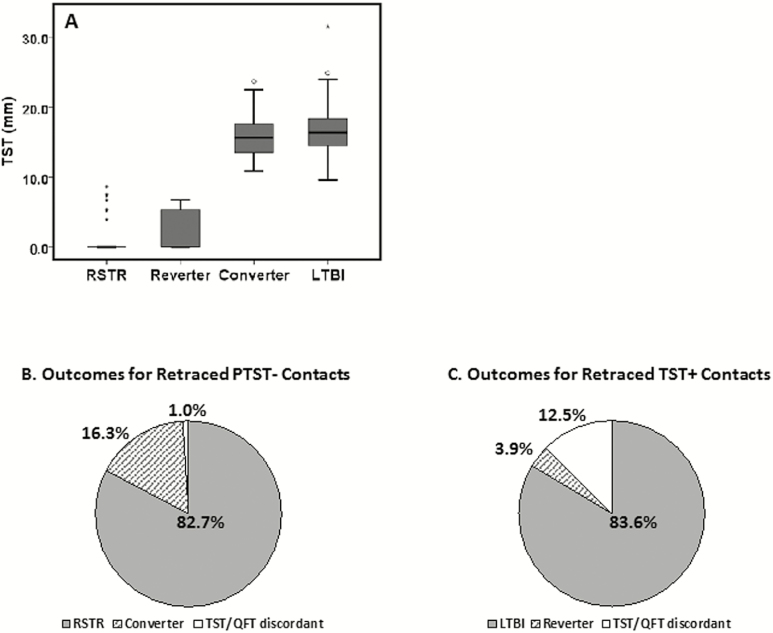
Results: Among PTST- with a definite classification, 82.7% were concordantly TST-/ quantiferon-TB Gold- (QFT-), and 16.3% converted to TST+/QFT+ LTBI. Among original LTBI contacts, 83.6% remained LTBI, and 3.9% reverted their TST and were QFT-. Although TST and QFT concordance was high (κ = 0.78), 1.0% of PTST and 12.5% of original LTBI contacts could not be classified due to discordant TST and QFT results. Epidemiological variables did not differ between retraced PTST- and LTBI contacts.
Conclusion: Resistance to LTBI, defined by repeatedly negative TST and IGRA, in adults who have had close contact with pulmonary TB patients living in TB-endemic areas, is a stable outcome of M.tb exposure. Repeated longitudinal measurements with 2 different immune assays and extended follow-up provide enhanced discriminatory power to identify this resister phenotype and avoid misclassification. Resisters may use immune mechanisms to control aerosolized M.tb that differ from those used by persons who develop "classic" LTBI.
Keywords: TB exposure; TB outcomes; case-contact study; resistance to infection.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO global surveillance and monitoring project. JAMA 1999; 282:677–86. - PubMed
-
- Hanifa Y, Grant AD, Lewis J, Corbett EL, Fielding K, Churchyard G. Prevalence of latent tuberculosis infection among gold miners in South Africa. Int J Tuberc Lung Dis 2009; 13:39–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
