

Opportunities for intervention: stroke treatments, disability and mortality in urban Tanzania
- PMID: 30165650
- PMCID: PMC6528701
- DOI: 10.1093/intqhc/mzy188
Opportunities for intervention: stroke treatments, disability and mortality in urban Tanzania
Abstract
Objective: Given the high post-stroke mortality and disability and paucity of data on the quality of stroke care in Sub-Saharan Africa, we sought to characterize the implementation of stroke-focused treatments and 90-day outcomes of neuroimaging-confirmed stroke patients at the largest referral hospital in Tanzania.
Design: Prospective cohort study.
Setting: Muhimbili National Hospital (MNH) in Dar es Salaam, July 2016-March 2017.
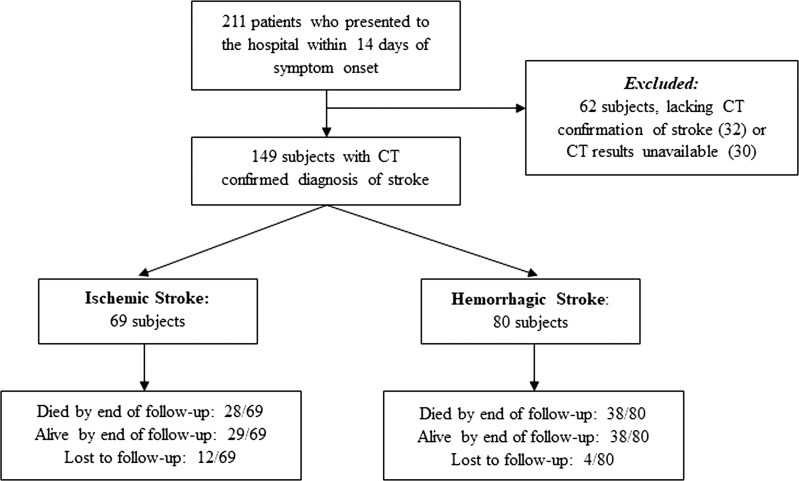
Participants: Adults with new-onset stroke (<14 days), confirmed by head CT, admitted to MNH.
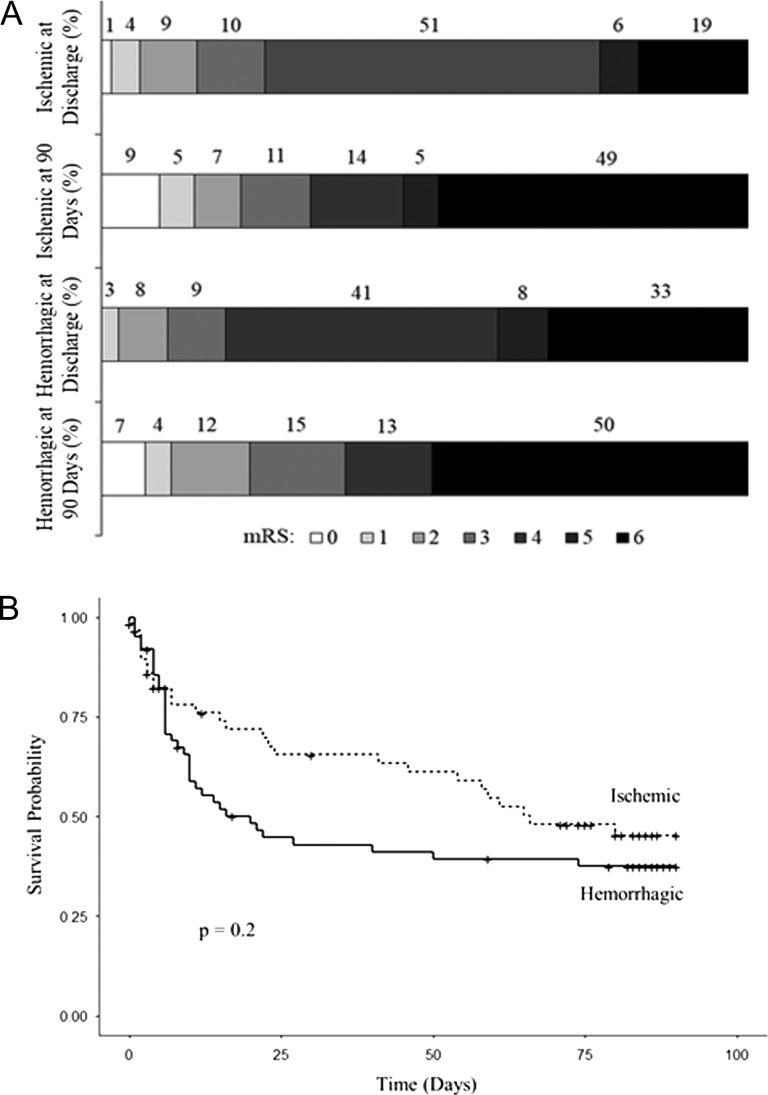
Main outcomes measures: Modified Rankin scale (mRS) and vital status.
Results: Of 149 subjects (mean age 57; 48% female; median NIH stroke scale (NIHSS) 19; 46% ischemic stroke; 54% hemorrhagic), implementation of treatments included: dysphagia screening (80%), deep venous thrombosis prophylaxis (0%), aspirin (83%), antihypertensives (89%) and statins (95%). There was limited ability to detect atrial fibrillation and carotid artery disease and no acute thrombolysis or thrombectomy. Of ischemic subjects, 19% died and 56% had severe disability (mRS 4-5) at discharge; 49% died by 90 days. Of hemorrhagic subjects, 33% died and 49% had severe disability at discharge; 50% died by 90 days. In a multivariable model, higher NIHSS score but not dysphagia, unconsciousness, or patient age was predictive of death by 90 days.
Conclusions: The 90-day mortality of stroke presenting at MNH is 50%, much higher than in higher income settings. Although severe stroke presentations are a major factor, efforts to improve the quality of care and prevent complications of stroke are urgently needed. Acute stroke interventions with low number needed to treat represent challenging long-term goals.
Keywords: Africa; developing countries; equity in healthcare; intracranial hemorrhage; ischemic stroke; mortality; needs assessment; patient outcomes; quality measurement.
© The Author(s) 2018. Published by Oxford University Press in association with the International Society for Quality in Health Care. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Similar articles
-
Safety of Intravenous Thrombolysis in Chronic Intracranial Hemorrhage: A Five-Year Multicenter Study.J Stroke Cerebrovasc Dis. 2018 Mar;27(3):620-624. doi: 10.1016/j.jstrokecerebrovasdis.2017.09.037. J Stroke Cerebrovasc Dis. 2018. PMID: 29100859
-
Quality of acute ischemic stroke care in Thailand: a prospective multicenter countrywide cohort study.J Stroke Cerebrovasc Dis. 2014 Feb;23(2):213-9. doi: 10.1016/j.jstrokecerebrovasdis.2012.12.001. Epub 2013 Jan 8. J Stroke Cerebrovasc Dis. 2014. PMID: 23305673
-
Effect of intravenous tirofiban and aspirin in reducing short-term and long-term neurologic deficit in patients with ischemic stroke: a double-blind randomized trial.Cerebrovasc Dis. 2010 Feb;29(3):275-81. doi: 10.1159/000275503. Epub 2010 Jan 15. Cerebrovasc Dis. 2010. PMID: 20090319 Clinical Trial.
-
Intravenous thrombolysis for acute ischemic stroke associated to extracranial internal carotid artery occlusion: the ICARO-2 study.Cerebrovasc Dis. 2012;34(5-6):430-5. doi: 10.1159/000345081. Epub 2012 Dec 1. Cerebrovasc Dis. 2012. PMID: 23207482
-
Symptomatic intracranial hemorrhage following intravenous thrombolysis for acute ischemic stroke: a critical review of case definitions.Cerebrovasc Dis. 2012;34(2):106-14. doi: 10.1159/000339675. Epub 2012 Aug 1. Cerebrovasc Dis. 2012. PMID: 22868870 Review.
Cited by
-
Measuring Ambulation, Motor, and Behavioral Outcomes with Post-stroke Fluoxetine in Tanzania: The Phase II MAMBO Trial.Am J Trop Med Hyg. 2021 Dec 6;106(3):970-978. doi: 10.4269/ajtmh.21-0653. Am J Trop Med Hyg. 2021. PMID: 34872059 Free PMC article. Clinical Trial.
-
Younger age of stroke in low-middle income countries is related to healthcare access and quality.Ann Clin Transl Neurol. 2022 Mar;9(3):415-427. doi: 10.1002/acn3.51507. Epub 2022 Feb 9. Ann Clin Transl Neurol. 2022. PMID: 35142101 Free PMC article.
-
Relationship Between Pain and Disability Among Stroke Patients.Anesth Pain Med. 2023 May 5;13(3):e136330. doi: 10.5812/aapm-136330. eCollection 2023 Jun. Anesth Pain Med. 2023. PMID: 38021327 Free PMC article.
-
Predictors of 30-day and 90-day mortality among hemorrhagic and ischemic stroke patients in urban Uganda: a prospective hospital-based cohort study.BMC Cardiovasc Disord. 2020 Oct 8;20(1):442. doi: 10.1186/s12872-020-01724-6. BMC Cardiovasc Disord. 2020. PMID: 33032527 Free PMC article.
-
Symmetric CTA Collaterals Identify Patients with Slow-progressing Stroke Likely to Benefit from Late Thrombectomy.Radiology. 2022 Feb;302(2):400-407. doi: 10.1148/radiol.2021210455. Epub 2021 Nov 2. Radiology. 2022. PMID: 34726532 Free PMC article.
References
-
- Strong K, Mathers C, Bonita R. Preventing stroke: saving lives around the world. Lancet Neurol 2007;6:182–7. - PubMed
-
- Feigin VL, Lawes CM, Bennett DA et al. . Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review. Lancet Neurol 2009;8:355–69. - PubMed
-
- Langhorne P, de Villiers L, Pandian JD. Applicability of stroke-unit care to low-income and middle-income countries. Lancet Neurol 2012;11:341–8. - PubMed
-
- Walker R, Whiting D, Unwin N et al. . Stroke incidence in rural and urban Tanzania: a prospective, community-based study. Lancet Neurol 2010;9:786–92. - PubMed
-
- Guida P, Iacoviello M, Passantino A et al. . Intra-hospital correlations among 30-day mortality rates in 18 different clinical and surgical settings. Int J Qual Health Care 2016;28:793–801. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
