

The association of calcium oxalate deposition in kidney allografts with graft and patient survival
- PMID: 30165691
- PMCID: PMC7849934
- DOI: 10.1093/ndt/gfy271
The association of calcium oxalate deposition in kidney allografts with graft and patient survival
Erratum in
-
The association of calcium oxalate deposition in kidney allografts with graft and patient survival.Nephrol Dial Transplant. 2021 Mar 29;36(4):747. doi: 10.1093/ndt/gfy364. Nephrol Dial Transplant. 2021. PMID: 30590582 Free PMC article. No abstract available.
Abstract
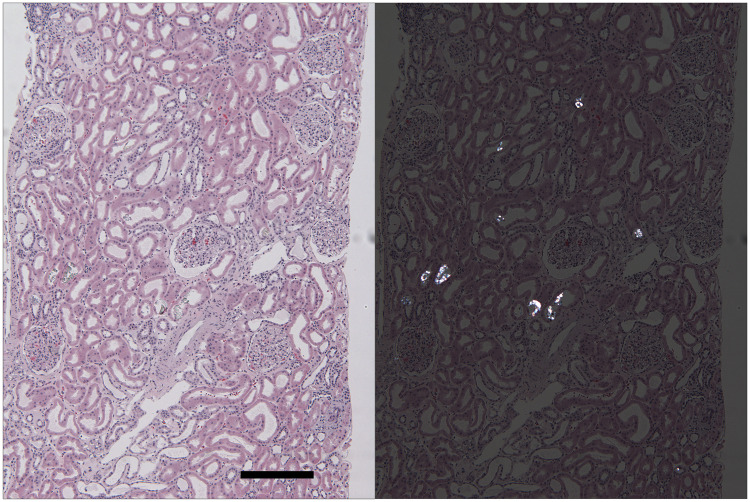
Background: Whether calcium oxalate (CaOx) deposition in kidney allografts following transplantation (Tx) adversely affects patient outcomes is uncertain, as are its associated risk factors.
Methods: We performed a retrospective cohort study of patients who had kidney allograft biopsies performed within 3 months of Tx at Brigham and Women's Hospital and examined the association of CaOx deposition with the composite outcome of death or graft failure within 5 years.
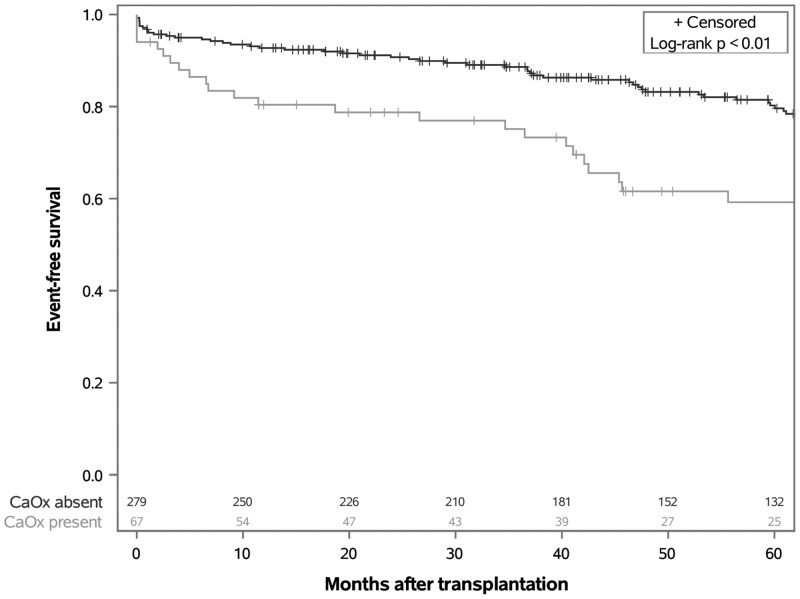
Results: Biopsies from 67 of 346 patients (19.4%) had CaOx deposition. In a multivariable logistic regression model, higher serum creatinine [odds ratio (OR) = 1.28 per mg/dL, 95% confidence interval (CI) 1.15-1.43], longer time on dialysis (OR = 1.11 per additional year, 95% CI 1.01-1.23) and diabetes (OR = 2.26, 95% CI 1.09-4.66) were found to be independently associated with CaOx deposition. CaOx deposition was strongly associated with delayed graft function (DGF; OR = 11.31, 95% CI 5.97-21.40), and with increased hazard of the composite outcome after adjusting for black recipient race, donor type, time on dialysis before Tx, diabetes and borderline or acute rejection (hazard ratio 1.90, 95% CI 1.13-3.20).
Conclusions: CaOx deposition is common in allografts with poor function and portends worse outcomes up to 5 years after Tx. The extent to which CaOx deposition may contribute to versus result from DGF, however, cannot be determined based on our retrospective and observational data. Future studies should examine whether reducing plasma and urine oxalate prevents CaOx deposition in the newly transplanted kidney and whether this has an effect on clinical outcomes.
Keywords: biopsy; calcium oxalate; graft survival; kidney transplantation; renal insufficiency.
© The Author(s) 2018. Published by Oxford University Press on behalf of ERA-EDTA. All rights reserved.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
