

Long-term efficacy and effectiveness of a behavioural and community-based exercise intervention (Urban Training) to increase physical activity in patients with COPD: a randomised controlled trial
- PMID: 30166322
- PMCID: PMC6203405
- DOI: 10.1183/13993003.00063-2018
Long-term efficacy and effectiveness of a behavioural and community-based exercise intervention (Urban Training) to increase physical activity in patients with COPD: a randomised controlled trial
Abstract
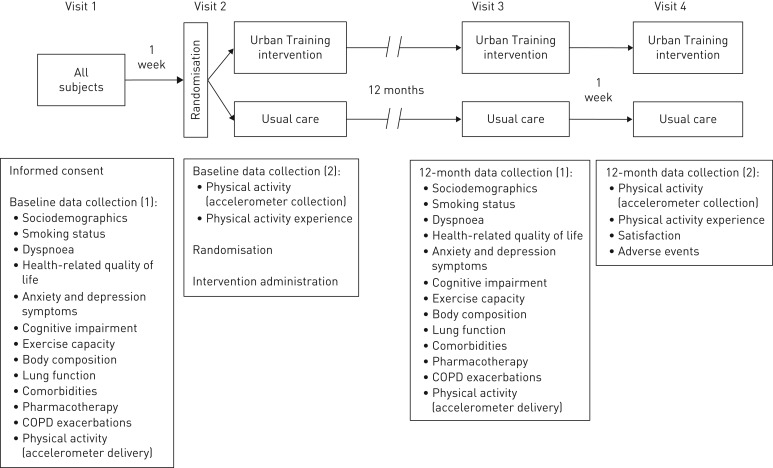
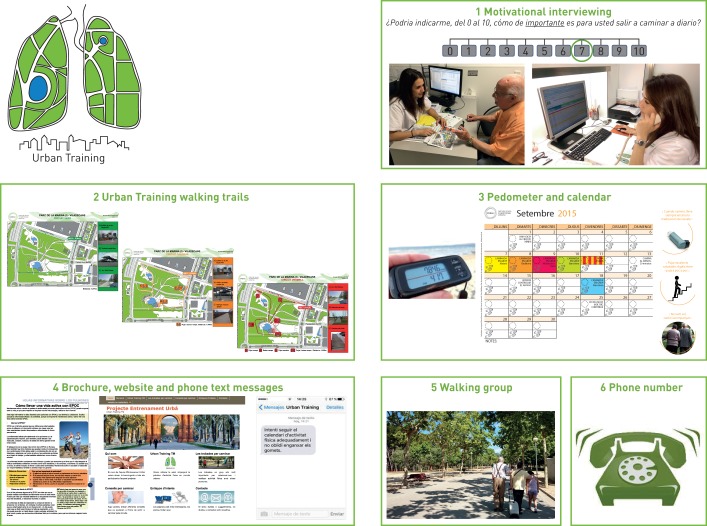
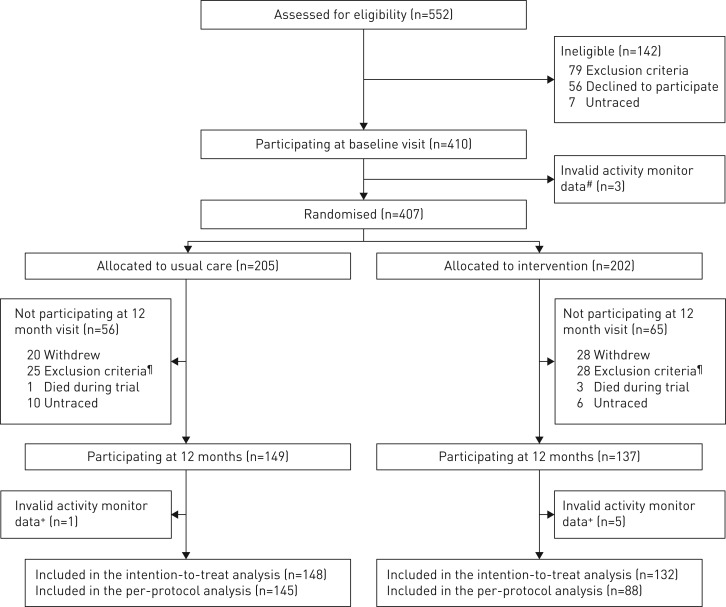
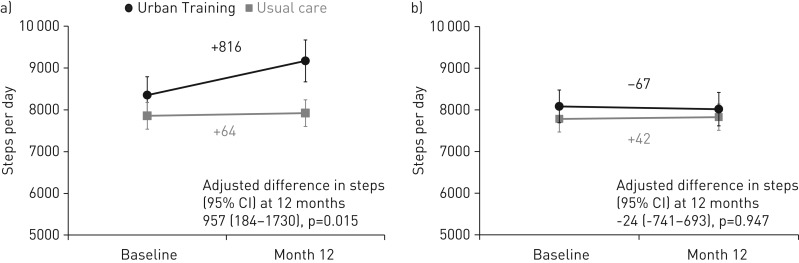
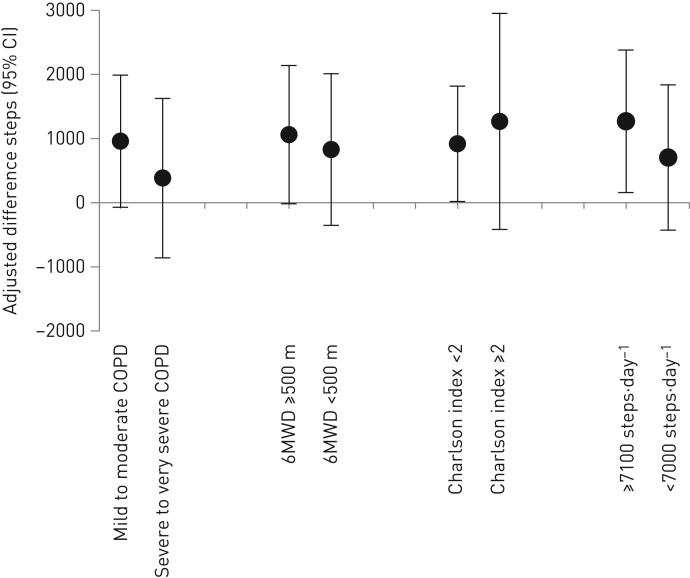
There is a need to increase and maintain physical activity in patients with chronic obstructive pulmonary disease (COPD). We assessed 12-month efficacy and effectiveness of the Urban Training intervention on physical activity in COPD patients.This randomised controlled trial (NCT01897298) allocated 407 COPD patients from primary and hospital settings 1:1 to usual care (n=205) or Urban Training (n=202). Urban Training consisted of a baseline motivational interview, advice to walk on urban trails designed for COPD patients in outdoor public spaces and other optional components for feedback, motivation, information and support (pedometer, calendar, physical activity brochure, website, phone text messages, walking groups and a phone number). The primary outcome was 12-month change in steps·day-1 measured by accelerometer.Efficacy analysis (with per-protocol analysis set, n=233 classified as adherent to the assigned intervention) showed adjusted (95% CI) 12-month difference +957 (184-1731) steps·day-1 between Urban Training and usual care. Effectiveness analysis (with intention-to-treat analysis set, n=280 patients completing the study at 12 months including unwilling and self-reported non-adherent patients) showed no differences between groups. Leg muscle pain during walks was more frequently reported in Urban Training than usual care, without differences in any of the other adverse events.Urban Training, combining behavioural strategies with unsupervised outdoor walking, was efficacious in increasing physical activity after 12 months in COPD patients, with few safety concerns. However, it was ineffective in the full population including unwilling and self-reported non-adherent patients.
Copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: A. Arbillaga-Etxarri has nothing to disclose. Conflict of interest: E. Gimeno-Santos has nothing to disclose. Conflict of interest: A. Barberan-Garcia has nothing to disclose. Conflict of interest: E. Balcells has nothing to disclose. Conflict of interest: M. Benet has nothing to disclose. Conflict of interest: E. Borrell has nothing to disclose. Conflict of interest: N. Celorrio has nothing to disclose. Conflict of interest: A. Delgado has nothing to disclose. Conflict of interest: C. Jané has nothing to disclose. Conflict of interest: A. Marin has nothing to disclose. Conflict of interest: C. Martín-Cantera has nothing to disclose. Conflict of interest: M. Monteagudo has nothing to disclose. Conflict of interest: N. Montellà has nothing to disclose. Conflict of interest: L. Muñoz has nothing to disclose. Conflict of interest: P. Ortega has nothing to disclose. Conflict of interest: D.A. Rodríguez has nothing to disclose. Conflict of interest: R. Rodríguez-Roisin reports grants from Almirall and Menarini, personal fees for advisory board work from Boehringer Ingelheim, Pearl Therapeutics and TEVA, personal fees for lecturinf from Novartis and Takeda, during the conduct of the study, all related to COPD. Conflict of interest: P. Simonet reports personal fees for speaking from Menarini, Gebro, Teva, Boehringer, Rovi, AstraZeneca and GSK, outside the submitted work. Conflict of interest: P. Torán-Monserrat has nothing to disclose. Conflict of interest: J. Torrent-Pallicer has nothing to disclose. Conflict of interest: P. Vall-Casas has nothing to disclose. Conflict of interest: J. Vilaró has nothing to disclose. Conflict of interest: J. Garcia-Aymerich reports personal fees for consulting and lecture fees paid to institution from AstraZeneca, personal fees for lecturing from Esteve and Chiesi, outside the submitted work.
Figures
Comment in
-
Whither pulmonary rehabilitation? Will alternative modes help or hurt?Eur Respir J. 2018 Oct 18;52(4):1801678. doi: 10.1183/13993003.01678-2018. Print 2018 Oct. Eur Respir J. 2018. PMID: 30337489 No abstract available.
References
-
- Leidy NK, Kimel M, Ajagbe L, et al. Designing trials of behavioral interventions to increase physical activity in patients with COPD: insights from the chronic disease literature. Respir Med 2014; 108: 472–481. - PubMed
-
- Singh S. One step at a time. Lifestyle physical activity interventions. Ann Am Thorac Soc 2016; 13: 586–587. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical