

The use of a subacromial spacer-inspace balloon in managing patients with irreparable rotator cuff tears
- PMID: 30166800
- PMCID: PMC6107884
- DOI: 10.1016/j.jor.2018.08.004
The use of a subacromial spacer-inspace balloon in managing patients with irreparable rotator cuff tears
Erratum in
-
Erratum regarding missing Declaration of Competing Interest statements in previously published articles.J Orthop. 2020 Dec 14;23:275. doi: 10.1016/j.jor.2020.12.003. eCollection 2021 Jan-Feb. J Orthop. 2020. PMID: 33746419 Free PMC article.
Abstract
Aim: The objective of this prospective non-randomized study was to establish the role of biodegradable sub-acromial spacer (InSpace™) insertion in the management of patients with massive irreparable rotator cuff tear by reporting beneficial effects on the pain relief and functional outcomes in these patients.
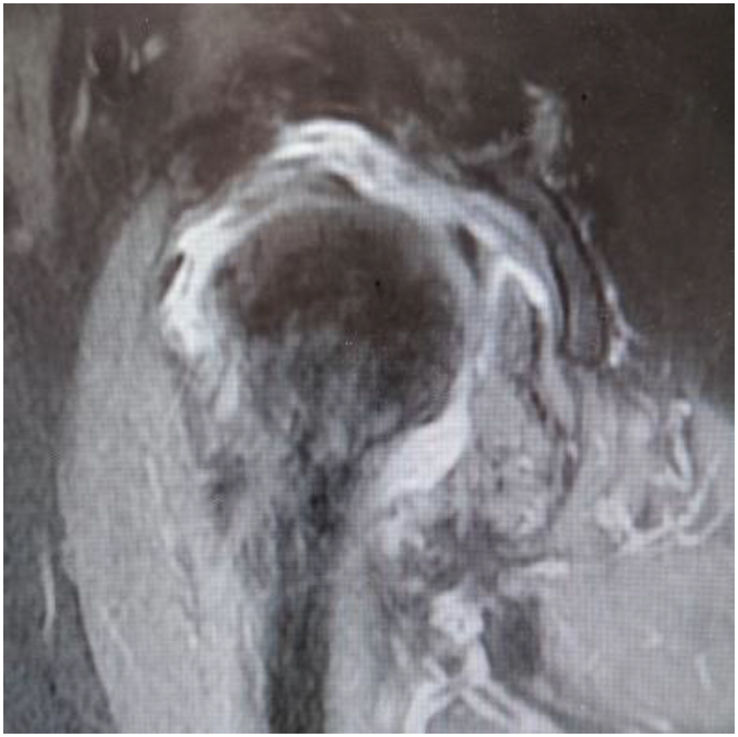
Methods: This is a prospective non-randomized study of patients treated for irreparable cuff tears during a period between January 2014 and November 2016.14 patients with symptomatic massive irreparable rotator cuff tears were managed with arthroscopic debridement and implantation of a biodegradable subacromial spacer and were followed up for at least one year (8-16 m). Inclusion criteria were patients with irreparable rotator cuff tears that failed the conservative management, with muscle retraction (Patte > stage 2), muscle atrophy, and fatty infiltration (Goutalier type 3). Patients with osteoarthritis grade 3 in the Hamada classification and/or without preserved passive motion were excluded from our study. Outcome measures included pre and postoperative, the range of motion, Constant and Oxford shoulder scores. The decision to perform surgery was made after failure of nonoperative treatment and rehabilitation (massive rotator cuff tear protocol, reading shoulder unit)for at least six months.
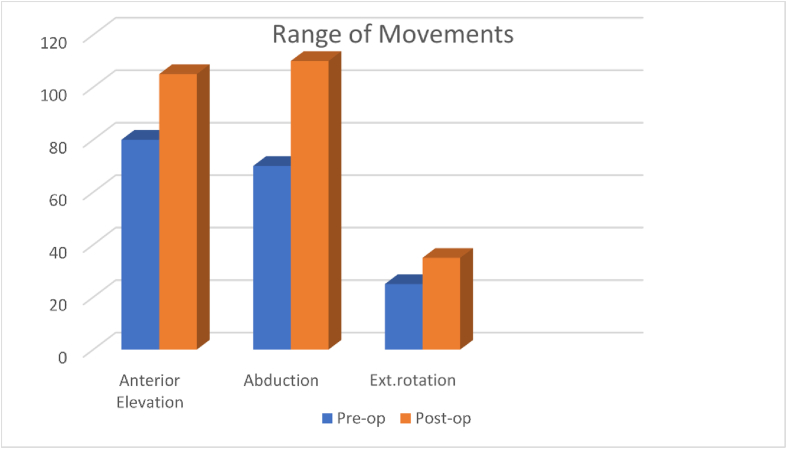
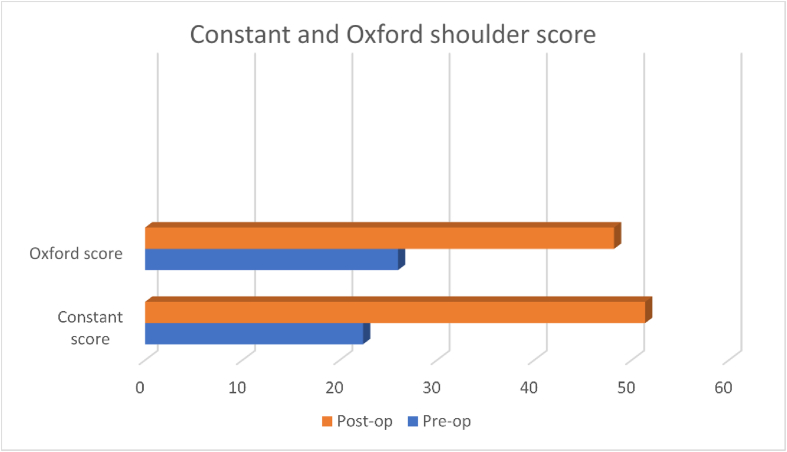
Results: Fourteen shoulders (14 patients, ten male four female) met the inclusion criteria. The mean age of patients was 76.2 (70-85) years. During the last follow-up (8-16 months mean 12.6 months), the range of motion was significantly increased in all patients with anterior elevation (from 80 to 105°), abduction (from 70 to 110°), and external rotation (from 25 to 35°). The mean Constant score was also significantly (P < 0.001) improved from 22.5 (13-33) preoperatively to 51.4 (30-64) at the last follow-up. The Oxford shoulder score improved from 26 preoperatively (21-28) to 48.2 postoperatively (34-56). No night pain following surgery and ADL increased by 40%, which is significant in these patients. No significant perioperative complications were found except for one patient who had a spacer migration. However, no action was required in that case.
Conclusions: Arthroscopic implantation of a subacromial spacer for irreparable rotator cuff tear resulted in a noticeable improvement in pain relief and shoulder function at a mean 12.6 months follow up. It is a quick, safe and a minimally invasive procedure that is suitable for elderly patients with irreparable cuff tears and medical co-morbidities.
Keywords: Balloon; Inspace; Irreparable cuff tear; Shoulder arthroscopy; Subacromial space.
Figures

References
-
- Ricchetti E.T., Aurora A., Iannotti J.P., Derwin K.A., Scaffold Devices for rotator cuff re-pair. J Shoulder Elbow Surg. 2012;21:251–265. - PubMed
-
- Gupta A.K., Hug K., Berkoff D.J. Dermal tissue allograft for the repair of massive irreparable rotator cuff tears. Am J Sports Med. 2012;40(1):141–147. - PubMed
-
- Scheibel M., Lichtenberg S., Habermeyer P. Reversed arthroscopic subacromial de-compression for massive rotator cuff tears. J Shoulder Elbow Surg. 2004;13(3):272–278. [Internet] - PubMed
-
- Mori D., Funakoshi N., Yamashita F. Arthroscopic surgery of irreparable large or mas-sive rotator cuff tears with low-grade fatty degeneration of the infraspinatus: patch autograft procedure versus partial repair procedure. Arthrosc J Arthrosc Relat Surg. 2013;29(12):1911–1921. - PubMed
-
- Mihata T., McGarry M.H., Pirolo J.M., Kinoshita M., Lee T.Q. Superior capsule recon-struction to restore superior stability in irreparable rotator cuff tears: a biomechani-cal cadaveric study. Am J Sports Med. 2012;40(10):2248–2255. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
